
Important: This article is for general informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Traumatic injuries vary widely in type and severity. Always follow the guidance of your treating physician, physiotherapist, or specialist. Do not alter your treatment plan without medical supervision.
Understanding Traumatic Injuries and the Recovery ChallengeRecovery at a Glance: The Six PillarsFollow Medical Advice: The Foundation of RecoveryWhy strict adherence mattersActive participation in your careMedical compliance checklistPrioritise Good Nutrition: Fuelling the Healing ProcessMacronutrients for recoveryHydrationManaging poor appetite during recoverySeek Mental Support: Psychological Dimension of RecoveryCommon psychological responses to traumatic injuryRole of professional psychological supportBuilding your support networkMove Mindfully: Safe, Graduated Physical RehabilitationPhases of physical rehabilitationPrinciples of mindful movement in recoveryPrioritise Sleep: When Your Body Does Most of Its Repair WorkSleep challenges common after traumatic injuryManaging Pain Effectively During RecoveryA multi-modal approach to pain managementFrequently Asked QuestionsWhat are the most common traumatic injuries?Why does healing take so long after a traumatic injury?Why is early treatment important after a traumatic accident?When should I contact my medical team during recovery?ConclusionDisclaimerReferences and Resources
Understanding Traumatic Injuries and the Recovery Challenge
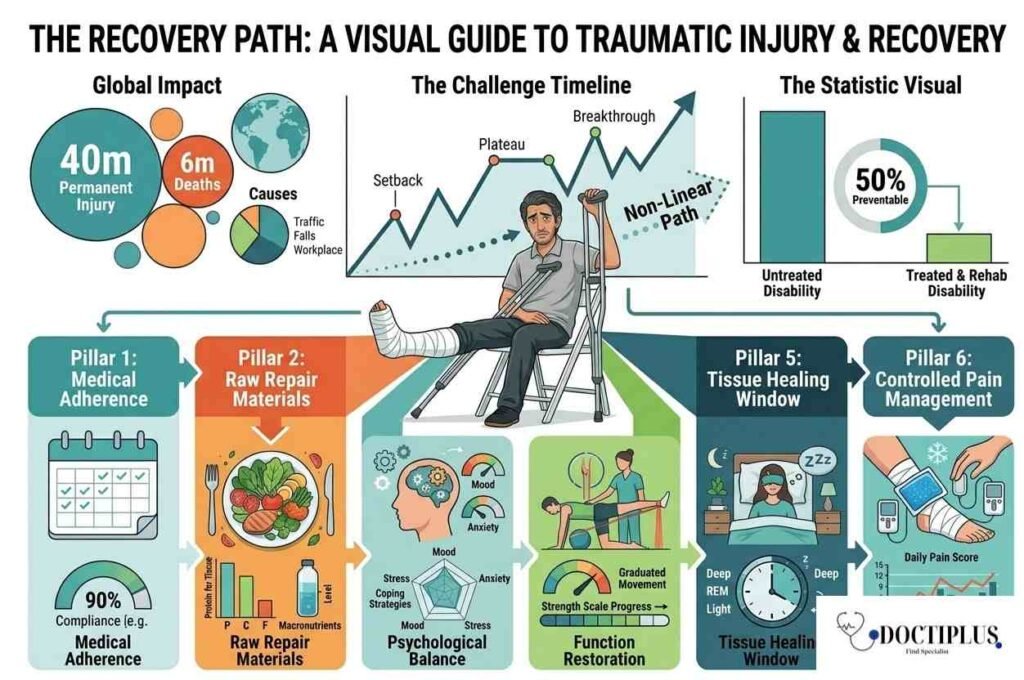
Traumatic injuries are among the most serious health events a person can experience. According to the National Institutes of Health (NIH), they rank among the leading causes of disability and death worldwide, affecting approximately 40 million people with permanent injury and contributing to nearly 6 million deaths each year. Whether caused by a road traffic accident, a fall, a workplace incident, a sports collision, or an act of violence, the physical and psychological aftermath of a traumatic injury can reshape a person’s life significantly.
Recovery from a traumatic injury is rarely linear. There are good days and setbacks, breakthroughs and plateaus. The path from injury to functional recovery depends on the type and severity of the injury, the quality of medical intervention, the patient’s baseline health, and crucially, the strategies and habits the patient uses to support healing throughout the process.
Key statistic: The World Health Organization estimates that up to 50 percent of disability from traumatic injury is preventable with timely, appropriate treatment and structured rehabilitation. How you manage recovery matters as much as the initial medical response.
Recovery at a Glance: The Six Pillars
| Pillar | What It Covers | Why It Matters |
| Medical compliance | Following prescribed treatment, medications, follow-ups | Prevents complications and setbacks |
| Nutrition | Macronutrients, micronutrients, hydration, meal timing | Provides raw materials for tissue repair |
| Mental health | PTSD, anxiety, emotional processing, professional support | Psychological state directly affects physical healing |
| Mindful movement | Graduated exercise, physiotherapy, safe strength building | Rebuilds function and prevents re-injury |
| Sleep and rest | Sleep quality, pain management at night, rest scheduling | Deep sleep is when most tissue repair occurs |
| Pain management | Medication, non-pharmacological methods, monitoring | Uncontrolled pain slows recovery and impairs sleep |
Follow Medical Advice: The Foundation of Recovery
No recovery strategy is more foundational than following the treatment plan established by your medical team. This sounds straightforward, but in practice it requires active discipline, particularly when you begin to feel better, and the temptation to reduce medication, skip follow-up appointments, or return to activity ahead of schedule becomes strong.
Why strict adherence matters
Traumatic injuries often involve damage that is not fully visible from the outside. A fracture that feels stable before it has properly consolidated can re-fracture under load. A healing ligament that is exposed to excessive stress too early may stretch beyond its functional range. An infection that appears to have resolved may be suppressed rather than eliminated if antibiotics are discontinued prematurely. Your medical team’s recommendations are calibrated to these biological realities, not simply to your subjective sense of how you feel.
Active participation in your care
Following advice does not mean passive compliance. Research published in the Journal of General Internal Medicine consistently shows that patients who actively participate in shared decision-making with their healthcare team achieve better outcomes than those who receive instructions without engagement. Ask your doctor to explain the reasoning behind each recommendation. Understand the goals of each medication, the purpose of each follow-up appointment, and the rationale for any restrictions on activity.
Do not adjust your treatment plan, reduce medications, or return to physical activity without explicit medical clearance. Even if you feel significantly better, the underlying tissue repair may not be complete. Early return to activity is one of the most common causes of re-injury and delayed recovery.
Medical compliance checklist
- Take all medications at the prescribed dose and time, including completing full antibiotic courses even if symptoms resolve
- Attend every scheduled follow-up appointment, including imaging reviews, physiotherapy assessments, and specialist consultations
- Report any new or worsening symptoms to your medical team promptly, rather than waiting for the next scheduled visit
- Keep a written log of your symptoms, functional abilities, and questions to bring to appointments
- Clarify the specific signs that should prompt an urgent contact with your care team, such as fever, increased swelling, loss of sensation, or wound changes
Prioritise Good Nutrition: Fuelling the Healing Process
The body cannot repair damaged tissue, rebuild bone, or restore immune function without adequate nutritional input. According to Drugs.com, the body relies on nutrients to mend wounds from injuries, surgeries, and pressure sores. There is no single healing diet, but a structured approach to nutrition can significantly accelerate recovery timelines and reduce the risk of complications, including wound infection, prolonged inflammation, and muscle loss during immobilisation.
Macronutrients for recovery
Protein is the most critical macronutrient for tissue repair. During the acute recovery phase following significant injury, protein requirements can increase to 1.5 to 2.0 grams per kilogram of body weight per day, well above the standard recommendation of 0.8 grams per kilogram for healthy adults. This elevated requirement supports the synthesis of collagen, which is essential for wound healing, and preserves lean muscle mass during periods of enforced rest.
Carbohydrates provide the energy substrate that cells use for repair processes. During recovery, dietary carbohydrate restriction can be counterproductive because it forces the body to use protein as an energy source rather than for tissue repair. Healthy fats, particularly omega-3 fatty acids found in oily fish, walnuts, and flaxseed, have well-documented anti-inflammatory properties that support the resolution of acute inflammation.
| Nutrient | Primary Role in Recovery | Best Food Sources |
| Protein | Tissue repair, collagen synthesis, immune function | Chicken, fish, eggs, Greek yogurt, legumes |
| Vitamin C | Collagen formation, antioxidant protection | Citrus fruit, peppers, strawberries, broccoli |
| Zinc | Wound healing, immune response, cell division | Red meat, shellfish, pumpkin seeds, legumes |
| Calcium | Bone repair and density | Dairy, fortified plant milks, sardines, kale |
| Vitamin D | Calcium absorption, immune modulation, muscle function | Sunlight, oily fish, eggs, fortified foods |
| Iron | Oxygen transport, energy, wound repair | Red meat, spinach, lentils, fortified cereals |
| Omega-3 fatty acids | Anti-inflammatory, cell membrane integrity | Salmon, mackerel, walnuts, flaxseed |
| Magnesium | Muscle and nerve function, protein synthesis | Nuts, seeds, dark chocolate, leafy greens |
Hydration
Water is involved in almost every metabolic process relevant to recovery, including nutrient transport to injury sites, waste product removal, temperature regulation, and joint lubrication. Dehydration impairs all of these functions. A general target during recovery is 35 to 40 ml of fluid per kilogram of body weight per day, with additional fluid required to replace losses from fever, increased metabolic activity, or drainage from wounds.
Managing poor appetite during recovery
Appetite suppression is common following traumatic injury, particularly in the acute phase. Pain, medication side effects, psychological distress, and reduced physical activity all contribute to reduced hunger. When appetite is poor, smaller and more frequent meals are preferable to three large meals, since they maintain a steady nutrient supply without requiring large volumes of food at once. High-calorie, nutrient-dense foods such as nut butters, full-fat dairy, avocado, and protein shakes can help meet elevated requirements without large meal volumes.
Avoid: Processed foods high in sugar and refined carbohydrates, excessive alcohol, and ultra-processed convenience foods. These promote systemic inflammation, impair immune function, and provide poor nutritional value relative to calorie content.
Seek Mental Support: Psychological Dimension of Recovery
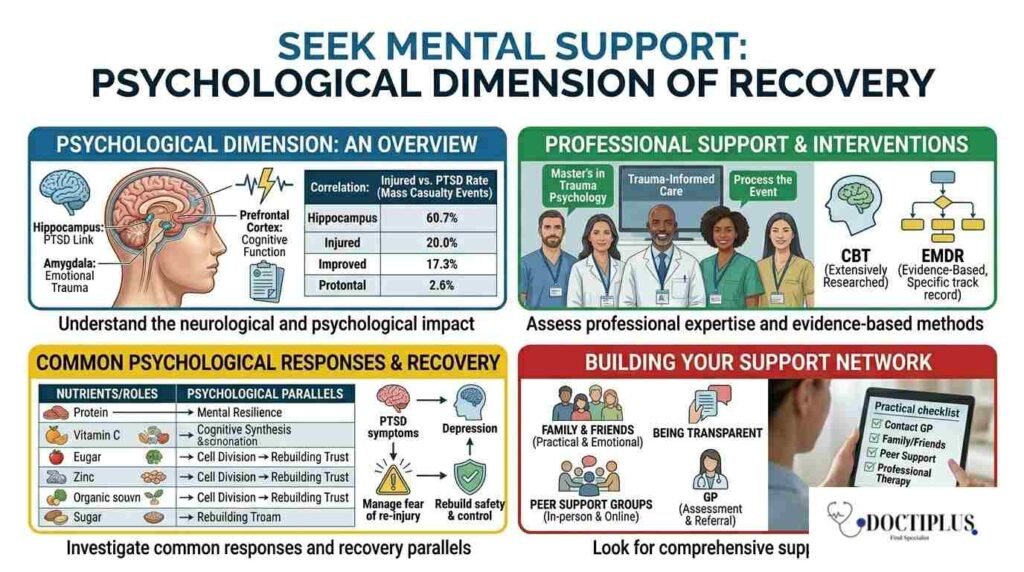
The mental health consequences of traumatic injury are frequently underestimated and undertreated. Research published in the Wiley Online Library demonstrates a strong correlation between the number of injured individuals in mass casualty events and the rate of post-traumatic stress disorder (PTSD) among survivors, highlighting how profoundly traumatic injuries affect psychological well-being alongside physical recovery. But the psychological impact is not limited to large-scale events. Even individual injuries from car accidents, workplace incidents, or sports trauma can produce significant and lasting mental health effects.
Common psychological responses to traumatic injury
| Nutrient | Primary Role in Recovery | Best Food Sources |
| Protein | Tissue repair, collagen synthesis, immune function | Chicken, fish, eggs, Greek yogurt, legumes |
| Vitamin C | Collagen formation, antioxidant protection | Citrus fruit, peppers, strawberries, broccoli |
| Zinc | Wound healing, immune response, cell division | Red meat, shellfish, pumpkin seeds, legumes |
| Calcium | Bone repair and density | Dairy, fortified plant milks, sardines, kale |
| Vitamin D | Calcium absorption, immune modulation, muscle function | Sunlight, oily fish, eggs, fortified foods |
| Iron | Oxygen transport, energy, wound repair | Red meat, spinach, lentils, fortified cereals |
| Omega-3 fatty acids | Anti-inflammatory, cell membrane integrity | Salmon, mackerel, walnuts, flaxseed |
| Magnesium | Muscle and nerve function, protein synthesis | Nuts, seeds, dark chocolate, leafy greens |
Role of professional psychological support
The psychological effects of traumatic injury ripple through overall well-being at every stage of life. According to Psych Degree Starter, professionals with a Master’s in Trauma Psychology are equipped with specialised training in trauma-informed care, enabling them to provide targeted support for the emotional and psychological dimensions of recovery. Trauma-informed therapists can help patients process the injury event itself, manage fear of re-injury, rebuild a sense of safety and control, and develop coping strategies that support both psychological and physical healing.
Cognitive behavioural therapy (CBT) is the most extensively researched psychological intervention for PTSD. It is recommended by clinical guidelines including those from the National Institute for Health and Care Excellence (NICE) and the American Psychological Association. Eye movement desensitisation and reprocessing (EMDR) is another evidence-based approach with a strong track record specifically for trauma-related disorders.
Building your support network
Professional therapy is not the only source of meaningful psychological support during recovery. Family members and close friends can provide practical and emotional support that significantly reduces the burden of the recovery process. Being transparent with those close to you about what you are experiencing, rather than minimising difficulties to protect others, allows them to provide targeted support. Peer support groups, either in person or online, can connect patients with others who have survived similar injuries, providing perspectives and coping strategies that professional support alone cannot offer.
Practical step: If you believe you may be experiencing symptoms of PTSD, depression, or significant anxiety following a traumatic injury, speak to your GP as a starting point. They can assess your symptoms and refer you to appropriate psychological support. You do not need to wait until symptoms become severe to seek help.
Move Mindfully: Safe, Graduated Physical Rehabilitation
Returning to physical activity after a traumatic injury requires careful calibration between doing enough to support recovery and avoiding the overexertion that causes re-injury or delays healing. Research referenced by the BBC notes that increasing your activity gradually is a smart way to keep your body from getting overloaded. Emphasising safe strength building and targeting the right muscle groups helps with recovery and lowers the risk of re-injury. This graduated approach, often formalised within a structured physiotherapy programme, is the clinical standard for physical rehabilitation following serious injury.
Phases of physical rehabilitation
| Phase | Focus | Typical Activities |
| Acute (Days 1-7) | Pain control, swelling reduction, protection | Rest, ice, compression, elevation (RICE); gentle range of motion if cleared |
| Sub-acute (Weeks 2-6) | Restore range of motion, reduce stiffness | Passive and active-assisted exercises, hydrotherapy, gentle stretching |
| Strengthening (Weeks 6-12) | Rebuild muscle strength and joint stability | Resistance exercises, physiotherapy-guided strengthening |
| Functional (Months 3-6) | Return to activity-specific function | Sport-specific training, occupational rehabilitation, balance work |
| Return to full activity (6+ months) | Full sport or work capacity | Graduated return under supervision, ongoing maintenance exercise |
Principles of mindful movement in recovery
Listen to pain signals: Pain during exercise is a signal that requires attention. Sharp, worsening, or joint-specific pain during movement should prompt you to stop and consult your physiotherapist or physician before continuing.g
Work with a physiotherapist: A qualified physiotherapist can design a rehabilitation programme that is specific to your injury type, current functional level, and recovery goals. Generic exercise programmes from the internet are not a substitute for individualised assessment.
Prioritise function over fitness: In the early and middle phases of recovery, the goal is restoring normal movement patterns and functional strength, not achieving fitness gains. Premature focus on high-intensity training is a common cause of re-injury
Include balance and proprioception work: Traumatic injuries to joints, particularly the ankle, knee, and shoulder, commonly impair proprioception, the body’s sense of joint position. Targeted balance exercises are essential for a safe return to activity.
Progress by symptoms, not by calendar: Recovery timelines are guides, not guarantees. Progress to the next phase of rehabilitation when you have achieved the functional benchmarks for the current phase, not simply because a certain number of weeks have elapsed
Prioritise Sleep: When Your Body Does Most of Its Repair Work
Sleep is not passive rest. It is the primary period during which the body performs most of its tissue repair, immune regulation, and hormonal restoration. Human growth hormone, which drives muscle and tissue repair, is released predominantly during deep slow-wave sleep. Inflammatory cytokines that coordinate healing are regulated during sleep. Disrupted or insufficient sleep therefore directly impairs the biological processes that recovery depends on.
Sleep challenges common after traumatic injury
- .Pain-related sleep disruption: Uncontrolled pain is the most common barrier to restorative sleep after traumatic injury. Work with your medical team to ensure pain management is adequate for nighttime as well as daytime.
- Positional discomfort: Injuries to the spine, shoulder, or hip may make comfortable sleeping positions difficult. A physiotherapist or occupational therapist can advise on positioning aids and pillow support.
- Medication effects: Some medications used in injury management, including certain pain relievers and corticosteroids, can affect sleep architecture. Discuss sleep disturbances related to medication with your prescribing physician.
- PTSD-related sleep disturbance: Nightmares, hyperarousal, and difficulty falling asleep are common in trauma-related psychological conditions and require targeted psychological intervention alongside physical recovery support.
| Sleep support strategy | How it helps recovery |
| Keep a consistent sleep and wake time | Stabilises circadian rhythm and growth hormone release |
| Keep bedroom cool and dark | Supports the core temperature drop needed for deep sleep |
| Avoid screens 60 minutes before bed | Reduces melatonin suppression from blue light |
| Take pain medication at a time that optimises nighttime coverage | Reduces nocturnal pain that wakes you |
| Use positioning aids for injured areas | Reduces discomfort from lying in fixed positions |
| Practice relaxation techniques before sleep | Lowers sympathetic nervous system activation before sleep |
| Discuss persistent insomnia with your GP | May indicate untreated pain, PTSD, or depression requiring intervention |
Managing Pain Effectively During Recovery
Pain is both a symptom and a barrier to recovery. Uncontrolled pain limits the ability to sleep, participate in rehabilitation, maintain adequate nutrition, and sustain the positive psychological state that supports healing. Effective pain management is not about eliminating all discomfort, which is rarely achievable, but about keeping pain within a range that allows you to function, rest, and engage with your rehabilitation programme.
A multi-modal approach to pain management
| Method | Type | Best Used For |
| Prescribed analgesics (paracetamol, NSAIDs, opioids) | Pharmacological | Acute and moderate pain, post-operative pain |
| Ice therapy (cryotherapy) | Non-pharmacological | Acute swelling, joint pain, post-exercise soreness |
| Heat therapy | Non-pharmacological | Muscle stiffness, chronic joint pain, muscle spasm |
| TENS (transcutaneous electrical nerve stimulation) | Non-pharmacological | Chronic musculoskeletal pain, nerve pain |
| Physiotherapy and manual therapy | Non-pharmacological | Joint and soft tissue pain, movement restriction |
| Cognitive behavioural therapy for pain (CBT-P) | Psychological | Chronic pain, pain catastrophising, fear of movement |
| Breathing and relaxation techniques | Psychological and physical | Acute pain management, anxiety-related pain amplification |
| Acupuncture | Complementary | Certain musculoskeletal pain types, as an adjunct to primary treatment |
t
Important: Opioid analgesics prescribed for acute traumatic pain carry a risk of dependency with prolonged use. Follow your prescribing physician’s guidance on dosage duration and tapering. Do not share or self-prescribe opioid medications, and discuss any concerns about pain management or medication dependence with your medical team promptly.
Frequently Asked Questions
What are the most common traumatic injuries?
- Traumatic injuries that most frequently result in emergency presentations and long-term rehabilitation include fractures of the long bones (femur, tibia, humerus), traumatic brain injury (TBI), spinal cord injuries, burns, soft tissue injuries, including ligament and tendon damage, and internal organ injuries. Road traffic accidents, falls from height, workplace incidents, and contact sports are the most common causes. Severity ranges from injuries that resolve within weeks to those requiring lifelong management.
Why does healing take so long after a traumatic injury?
- The duration of recovery reflects the biological complexity of tissue repair. Bone fractures require new bone formation across the fracture gap, a process that typically takes 6 to 12 weeks for initial union and up to a year for full remodelling. Tendon and ligament repairs are slower still, partly because these tissues have relatively poor blood supply. Inflammation, which is a necessary part of healing, also consumes significant metabolic resources and can delay recovery if it becomes chronic. Psychological factors, including pain catastrophising and fear of re-injury, are also established contributors to prolonged recovery in research literature.
Why is early treatment important after a traumatic accident?
- Early treatment serves several functions simultaneously. It prevents the escalation of injuries that may not be immediately apparent, such as intracranial haemorrhage, internal bleeding, or compartment syndrome. It initiates the inflammatory cascade in an optimal environment rather than a compromised one. It allows early mobilisation and rehabilitation in cases where this is appropriate, which research consistently shows produces better functional outcomes than a delayed start. And it creates a documented medical record from the time of injury, which is important for both clinical management and any insurance or legal processes that may follow.
When should I contact my medical team during recovery?
- Contact your medical team promptly if you experience any of the following: increasing pain rather than gradual improvement, fever or signs of infection including redness, warmth, swelling, or discharge at an injury site, sudden new neurological symptoms such as numbness, tingling, or weakness, significant mood changes including persistent low mood, thoughts of self-harm, or symptoms of PTSD, or any concern that your recovery trajectory has changed. Do not wait for a scheduled appointment if something feels wrong.
Conclusion
Healing from a traumatic injury demands patience, consistency, and a willingness to attend to every dimension of well-being simultaneously. Physical repair depends not only on medical intervention but on the nutritional substrate that supports it, the sleep that enables it, the psychological stability that sustains engagement with rehabilitation, and the graduated physical activity that restores function safely.
Every person’s recovery is individual. The timeline that applies to someone else’s injury will not necessarily apply to yours. What is universal is that the quality of your engagement with it significantly influences the quality of your recovery. Small, consistent steps, following your treatment plan, eating well, sleeping adequately, seeking mental health support when needed, and moving carefully and progressively, accumulate into the meaningful recovery that may feel far away in the early days after a serious injury.
You are not just healing from an injury. You are rebuilding your capacity to live fully. Give yourself the time, support, and resources that the process deserves.
Disclaimer
This article is provided for general informational and educational purposes only. It is not intended to constitute medical advice and should not be used as a substitute for consultation with a qualified physician, physiotherapist, psychologist, or other licensed healthcare professional. Traumatic injuries vary considerably in type, severity, and appropriate management. Individual recovery timelines and treatment approaches depend on factors that can only be assessed through direct clinical evaluation. Information in this article reflects published evidence and clinical guidelines available at the time of writing and may not encompass the most recent research or clinical recommendations. Always consult your treating healthcare team before making changes to your treatment, medication, diet, or physical activity during recovery from a traumatic injury.
References and Resources
- GBD 2019 Diseases and Injuries Collaborators. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019. The Lancet, 396(10258), 1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
- Roth GA, et al. (2018). Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories. The Lancet, 392(10159), 1736–1788. https://doi.org/10.1016/S0140-6736(18)32203-7
- National Institutes of Health (NIH). Traumatic Injury Research. (No DOI available)
- Collins N. (2003). Nutrition and wound healing. Advances in Skin & Wound Care, 16(4), 189–192. https://doi.org/10.1097/00129334-200307000-00010
- Guo S, & DiPietro LA. (2010). Factors affecting wound healing. Journal of Dental Research, 89(3), 219–229. https://doi.org/10.1177/0022034509359125
- Barker LA, Gout BS, & Crowe TC. (2011). Hospital malnutrition: prevalence, identification and impact. International Journal of Environmental Research and Public Health, 8(2), 514–527. https://doi.org/10.3390/ijerph8020514
- Drugs.com. Wound Care and Nutrition. (No DOI available)
- Kessler RC, et al. (1995). Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry, 52(12), 1048–1060. https://doi.org/10.1001/archpsyc.1995.03950240066012
- Breslau N. (2009). The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma, Violence, & Abuse, 10(3), 198–210. https://doi.org/10.1177/1524838009334448
- NICE. (2018). Post-traumatic stress disorder (NG116). (No DOI available)
- Khan KM, et al. (2010). Physical activity and injuries. British Journal of Sports Medicine, 44(15), 1081–1087. https://doi.org/10.1136/bjsm.2010.073015
- Bleakley CM, et al. (2012). PRICE needs updating, should we call the POLICE? British Journal of Sports Medicine, 46(4), 220–221. https://doi.org/10.1136/bjsports-2011-090297
- Sherrington C, et al. (2019). Exercise for preventing falls in older people. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD012424.pub2
- Walker MP. (2017). Why We Sleep: Unlocking the Power of Sleep and Dreams. Scribner. (No DOI available)
- Irwin MR. (2015). Why sleep is important for health. Annual Review of Psychology, 66, 143–172. https://doi.org/10.1146/annurev-psych-010213-115205
- Spiegel K, Tasali E, Leproult R, & Van Cauter E. (2009). Effects of poor and short sleep on metabolism. Nature Reviews Endocrinology, 5(5), 253–261. https://doi.org/10.1038/nrendo.2009.23
- Chou R, et al. (2017). Systemic pharmacologic therapies for low back pain. Annals of Internal Medicine, 166(7), 480–492. https://doi.org/10.7326/M16-2458
- Turk DC, Wilson HD, & Cahana A. (2011). Treatment of chronic non-cancer pain. The Lancet, 377(9784), 2226–2235. https://doi.org/10.1016/S0140-6736(11)60402-9