Reputation doesn’t sit in a lobby like a framed award. It moves. It travels down hallways, slips into group texts, and shows up in the pause before a clinician answers a recruiter’s call. Top clinical talent doesn’t choose a job the way someone chooses a toaster. The stakes feel moral. The work touches bodies, families, error rates, and sleep. A hospital or clinic can post glossy mission statements all day and still lose the best people if its name triggers a wince in the professional grapevine. Reputation acts like a shortcut for risk, and clinicians live inside risk for a living.
Whisper Network Beats the Billboard
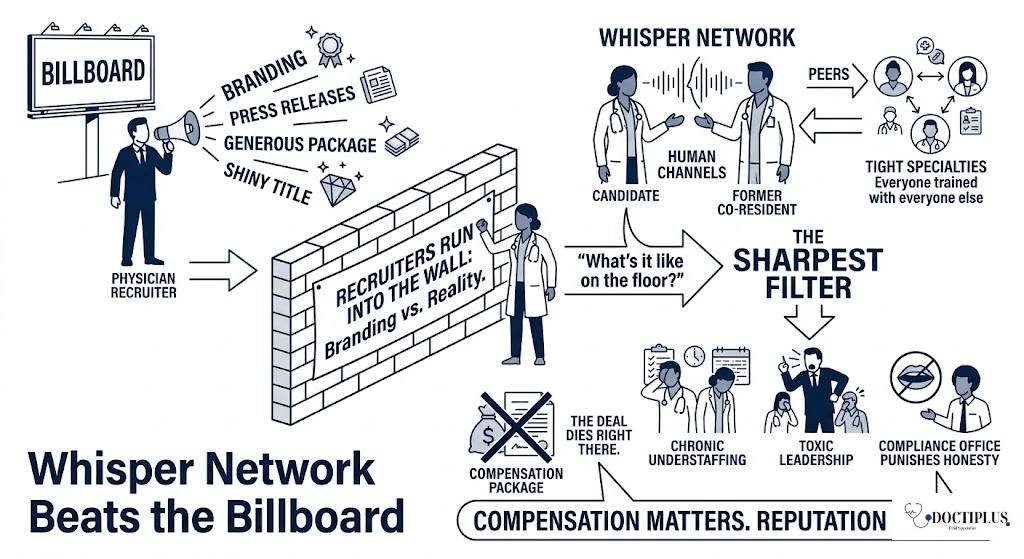
Reputation spreads through human channels, not press releases. The sharpest filter comes from peers who already know the place, especially in tight specialties where everyone trained with everyone else. This is where physician recruiters run into the wall between branding and reality. A recruiter can offer a generous package and a shiny title. Then a candidate calls a former co-resident and asks one question. “What’s it like on the floor?” If the answer includes chronic understaffing, toxic leadership, or a compliance office that punishes honesty, the deal dies right there. Compensation matters. Reputation decides whether compensation even gets a hearing.
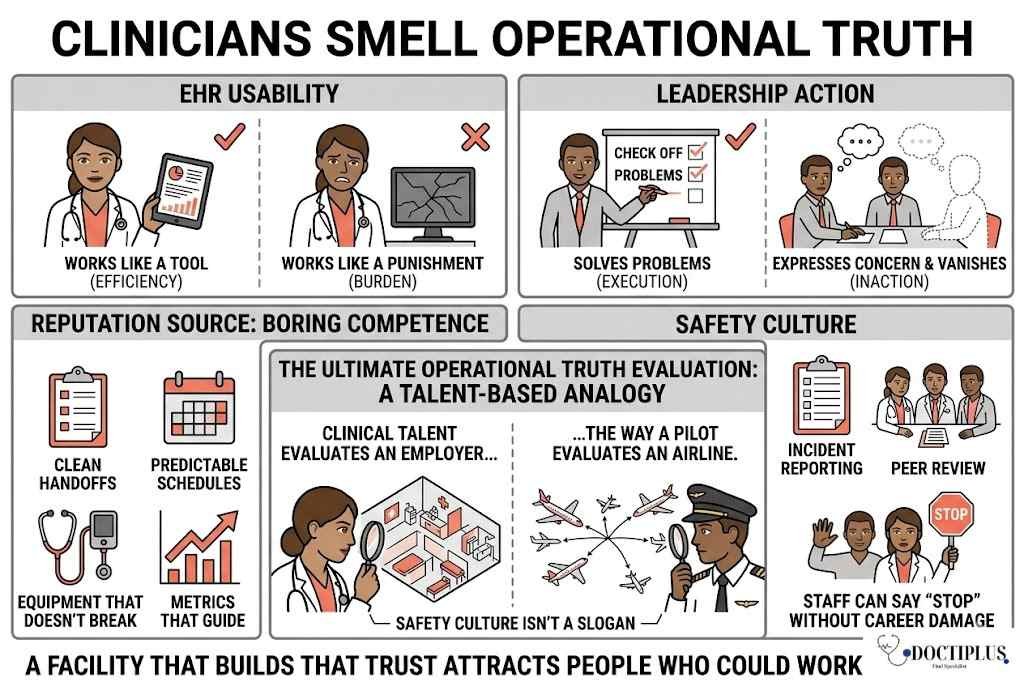
Clinicians Smell Operational Truth
Top clinicians don’t just treat patients. They read systems. They notice whether the EHR works like a tool or a punishment. They track whether leadership solves problems or expresses concern in meetings, only to vanish afterward. A strong reputation often comes from boring competence. Clean handoffs. Predictable schedules. Equipment that doesn’t break. Metrics that guide instead of threaten. Clinical talent evaluates an employer the way a pilot evaluates an airline. Safety culture isn’t a slogan. It shows up in incident reporting, peer review, and whether staff can say “stop” without career damage. A facility that builds that trust attracts people who could work anywhere.
Prestige Isn’t the Same as Trust
Some organizations chase prestige like it’s oxygen. Big names. Big buildings. Big ad campaigns. Then the inside story leaks. Burnout climbs. Turnover becomes normal. Patients wait. Clinicians notice the mismatch and judge it harshly because it signals vanity leadership. Trust grows from consistent behavior over time. It comes from fair call distribution, transparent promotion decisions, and leaders who show up when cases go sideways. Even research status doesn’t automatically fix the problem. A badge can attract early-career talent, then repel mid-career stars if the institution treats clinicians like replaceable parts.
Reputation Can Be Built, Then Kept
Reputation building starts with a blunt inventory. Exit interviews. Anonymous pulse surveys. Patient complaints sorted by root cause, not public relations panic. A facility that wants top talent must clean its house and do it loudly enough that staff believe the change. Speed matters. Adjust staffing models. Fund support roles that protect clinicians from clerical overload. Train managers to coach rather than intimidate. A single abusive leader can poison years of goodwill. Removing that leader often improves recruitment faster than any signing bonus. Reputation grows when daily life improves, then word spreads without anyone begging for it.
Conclusion
Top clinical talent seeks a reputation because it answers the most important questions job descriptions avoid. Does this facility provide safe care? Can coworkers behave like adults under pressure? Will leadership maintain standards or compromise for appearances? Clinicians won’t volunteer for an employer that adds avoidable dysfunction, since they already carry the emotional weight of outcomes. Smart companies see reputation as an operational asset, not a marketing tool. Fixed work and culture make recruitment easier because the story is easy to tell. Talent stays when internal experience matches exterior promise.
Disclaimer
This content is intended for informational and educational purposes only. It does not constitute medical, legal, or recruitment advice. Organizational practices, hiring outcomes, and clinician experiences can vary widely based on location, specialty, and regulatory environment. Healthcare institutions should consult qualified professionals and follow applicable laws, accreditation standards, and ethical guidelines when making staffing or operational decisions.
FAQs
1. Why is reputation so important in healthcare recruitment?
- Reputation acts as a shortcut for trust. Clinicians rely heavily on peer feedback and past experiences to judge whether a workplace is safe, ethical, and professionally supportive. A strong reputation reduces perceived risk and makes high-quality candidates more willing to engage.
2. Can a hospital improve its reputation quickly?
- Reputation can improve, but not instantly. Quick wins may come from removing toxic leadership or fixing major operational issues, but lasting reputation change requires consistent improvements in culture, staffing, and leadership behavior over time.
3. Do higher salaries compensate for poor reputation?
- In most cases, no. While compensation can attract attention, it rarely overcomes concerns about burnout, unsafe practices, or toxic work environments. Clinicians often prioritize working conditions and patient safety over financial incentives.
4. How do clinicians verify an organization’s reputation?
- Clinicians use informal networks, including colleagues, former classmates, and professional communities. They may also review turnover rates, patient outcomes, and online feedback, but peer-to-peer insights remain the most trusted source.
5. What is the biggest factor that damages reputation in healthcare settings?
- Consistent issues like understaffing, poor leadership, lack of support, and unsafe working conditions tend to cause the most harm. Even a single negative factor, such as an abusive manager, can significantly impact how an organization is perceived.
References
- Shanafelt, T. D., & Noseworthy, J. H. (2017). Executive leadership and physician well-being. Mayo Clinic Proceedings. https://doi.org/10.1016/j.mayocp.2016.10.004
- Dyrbye, L. N., et al. (2020). Burnout among healthcare professionals. Journal of Internal Medicine. https://doi.org/10.1111/joim.13131
- West, C. P., et al. (2018). Interventions to prevent and reduce physician burnout. The Lancet. https://doi.org/10.1016/S0140-6736(18)31517-X
- Edmondson, A. C. (1999). Psychological safety and learning behavior in work teams. Administrative Science Quarterly. https://doi.org/10.2307/2666999
- The Joint Commission. (2021). Workplace violence and safety in healthcare environments.
- Bodenheimer, T., & Sinsky, C. (2014). From triple to quadruple aim. Annals of Family Medicine. https://doi.org/10.1370/afm.1713