
- Social media invented a problem out of normal human skeleton architecture. Here is what hip dips actually are, why you have them, and why no workout routine will make them disappear.
Somewhere around 2018, the internet collectively decided that the slight inward curve between the hip bone and the upper thigh was a flaw. It got a name. “Hip dips.” It got a hashtag. It got thousands of workout videos promising to “fix” it. And millions of women who had never given a second thought to this particular section of their body suddenly had a new insecurity.
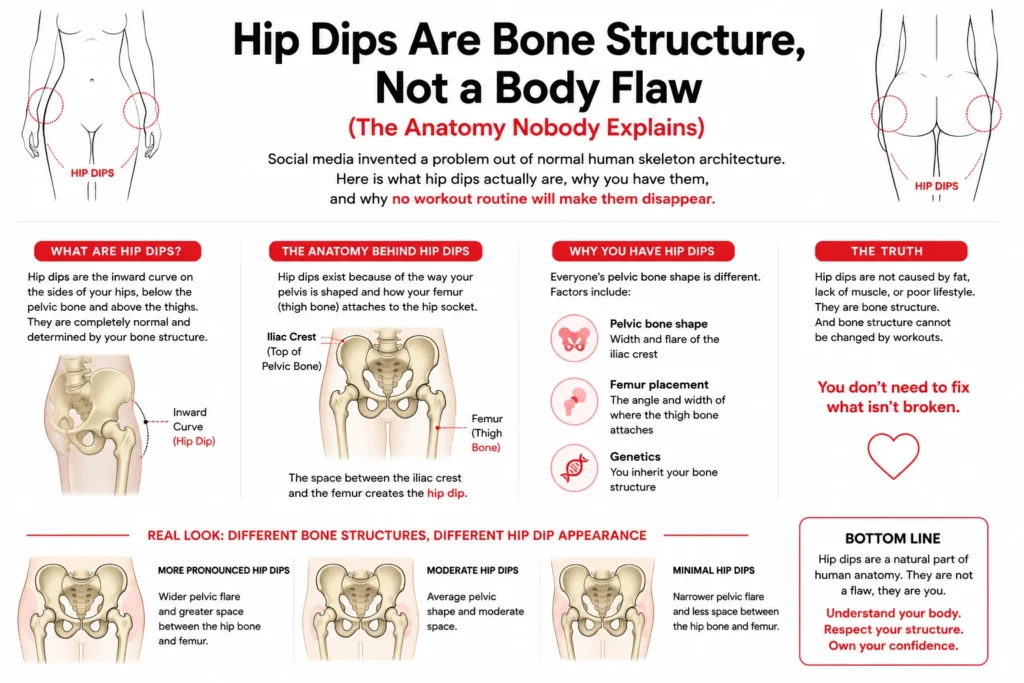
The irony is significant. Hip dips are not a condition. They are not a symptom. They are not the result of insufficient exercise, poor diet, or any lifestyle factor whatsoever. They are the visible result of skeletal anatomy, specifically the shape and angle of the pelvis and the position where the femur inserts into the hip socket. And no exercise, diet, or lifestyle change will alter that skeletal architecture.
What Creates the Indentation
The human pelvis is a complex bony structure with several key landmarks that influence the outer contour of the hips. The iliac crest (the top of the pelvis, where the hip bone flares outward) creates the widest point. Below that sits the greater trochanter of the femur (the bony knob at the top of the thigh bone where it connects to the hip socket).

The “hip dip” is the area between these two bony landmarks. In everyone, the soft tissue in this zone consists of the gluteus medius muscle, the tensor fasciae latae muscle, and a variable amount of fat. In some women, the combination of their specific pelvic width, the angle of the femoral neck, the depth of the hip socket, and the amount of muscle and fat overlaying this region creates a smooth, continuous curve from waist to thigh. In others, the skeletal geometry creates a visible indentation.
According to the American Council on Exercise, body shape and fat distribution are primarily determined by genetic and skeletal factors. The specific width of the ilium, the angle at which the femur meets the pelvis, and the depth of the acetabulum (hip socket) vary from person to person and are established during skeletal development. These are not modifiable through exercise.
Two women of identical height, weight, and body fat percentage can have dramatically different hip contours purely because their skeletons are shaped differently. One has wider iliac crests relative to her greater trochanters, creating a visible dip. The other has a more continuous curve. Neither is more correct or healthier than the other. They are different skeletal blueprints producing different silhouettes.
Why Workouts Cannot “Fix” Them
The fitness content around hip dips almost always targets the gluteus medius, the fan shaped muscle that sits on the outer surface of the pelvis in the exact zone where the dip appears. The logic seems sound: build the muscle, fill the dip.

The problem is anatomical. The gluteus medius is a relatively thin muscle that sits directly on bone. Even with significant hypertrophy (muscle growth), the volume it adds to this region is modest compared to the depth of the indentation in women whose skeletal anatomy creates a pronounced dip. Building the gluteus medius is excellent for hip stability, pelvic alignment, and athletic performance. It may slightly soften the appearance of a mild dip. But it will not fill in a dip that is determined by the distance between two bony prominences.
This is the same reason that no amount of calf raises will change the shape of the ankle bone, and no amount of forearm curls will change the width of the wrist. The muscle sits on top of the skeleton. It does not reshape the skeleton.
Research from the National Institutes of Health on body composition and regional fat distribution confirms that localized muscle development can change the surface contour of an area to a limited degree, but the underlying skeletal architecture remains the primary determinant of shape. Spot reduction of fat is not possible, and spot enhancement of contour through muscle growth has significant anatomical limits dictated by where muscles attach, how thick they can reasonably become, and what bony structures they are covering.
The Fat Distribution Variable
Fat does play a secondary role in hip dip visibility. Women who naturally store more fat in the lateral hip and upper thigh region tend to have a smoother curve across this zone because the fat fills in the indentation between the bony landmarks. Women who store fat preferentially in other areas (abdomen, lower thigh, back) may have less padding in the hip dip zone, making the skeletal contour more visible.
This explains why some women notice their hip dips becoming more or less prominent with weight fluctuation. Gaining weight may partially fill the area (along with adding fat everywhere else). Losing weight may make the dip more visible as the overlying fat thins. Neither scenario represents the dips getting “worse” or “better.” The skeleton did not change. The padding over it did.
This fat distribution pattern is governed by genetics and hormonal signaling, not by diet composition or exercise selection. The body deposits and withdraws fat from genetically predetermined locations in a genetically predetermined sequence. Targeted exercise in the hip dip region burns calories systemically. It does not instruct the body to deposit fat specifically in the indentation.
How Social Media Manufactured an Insecurity
Hip dips have existed for as long as human pelvises have existed. They appear in classical paintings, anatomical illustrations, and photographs from every era. They were not considered a flaw until social media algorithms identified them as a category of content that generated engagement.
The engagement loop works like this: create awareness of a “problem” most people had not noticed, offer a solution (workout program, supplement, device), collect views and clicks as people search for the fix, and repeat. The content that performs best is the content that creates the sharpest sense of inadequacy, because inadequacy drives searches, and searches drive revenue.
The result is that millions of women now scrutinize a section of their body that is functioning exactly as their anatomy dictates, believing that something is wrong because an algorithm told them so.
For anyone already deep in the comparison cycle, stepping back and looking at the actual anatomy, the actual variation, and the full range of options available (from acceptance to targeted exercise to body contouring) can replace the anxiety with clarity. This detailed guide to understanding hip dips and the full spectrum of approaches covers the anatomy, the lifestyle strategies, and the realistic expectations for each.
What Actually Matters
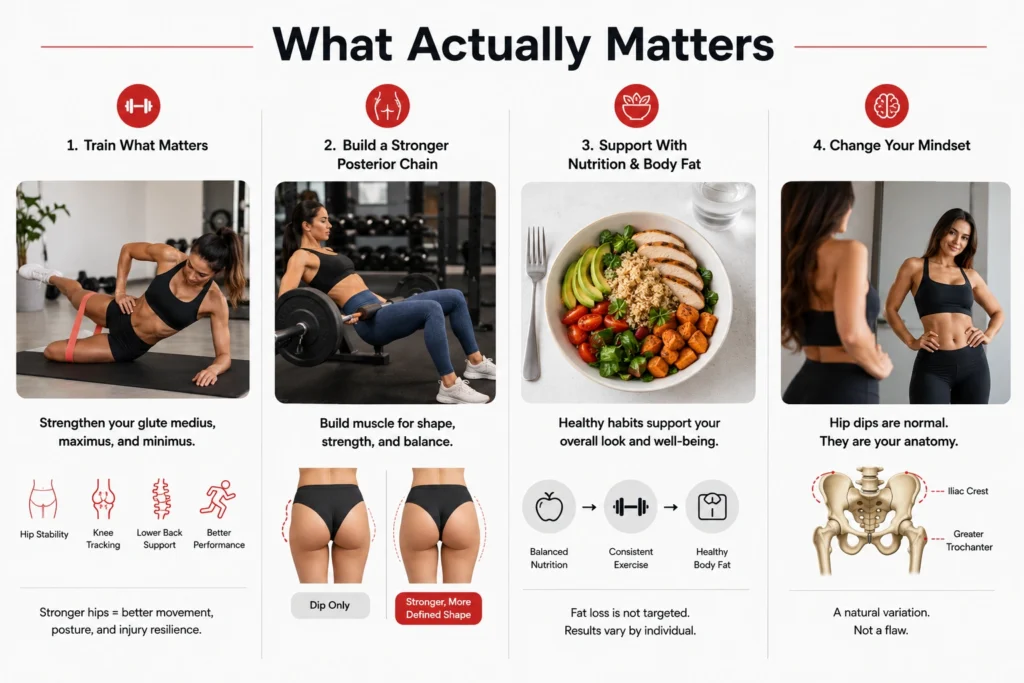
The gluteus medius is worth training. Not to fix hip dips, but because it is a critical muscle for hip stability, knee tracking, lower back support, and efficient movement in every direction. Weak glute medius muscles contribute to IT band syndrome, knee valgus, hip pain, and lower back dysfunction. Strengthening them improves posture, athletic performance, and injury resilience.
Building the glute maximus and minimus alongside the medius creates a stronger, more balanced posterior chain that changes the overall contour of the hip and buttock region. The result may not eliminate the dip, but it creates a more muscular, defined silhouette that most women find more satisfying than the dip alone suggested.
Body fat management through balanced nutrition and consistent exercise supports overall health and can modestly influence how prominent the dip appears, depending on individual fat distribution patterns. But pursuing aggressive fat loss specifically to change hip contour is a losing strategy, because the body does not allow selective fat loss from targeted regions.
The most productive mental shift is the simplest one: hip dips are not something that happened to you. They are how you are built. Pelvic anatomy varies enormously across the human population, and the indentation between the iliac crest and the greater trochanter is one of the most visible expressions of that variation. It has always been there. The only thing that changed is that someone decided to name it and call it a problem.
It was never a problem. It was always just a hip.
References:
- American Council on Exercise – What Are Hip Dips?
- National Institutes of Health – Body Fat Distribution and Genetics
- National Institutes of Health – Gluteus Medius Muscle Function
- Cleveland Clinic – Hip Anatomy Overview
- Johns Hopkins Medicine – Pelvis Anatomy
- NIH – Skeletal Structure and Human Body Shape Research
- Healthline – Hip Dips Explained by Anatomy
- Medical News Today – What Causes Hip Dips?
- Harvard Health – Why Spot Reduction Does Not Work
- Verywell Fit – Hip Dips and Pelvic Structure Explained