
Most people assume better vision means stronger glasses or a new prescription. But eye care has moved far beyond basic correction. Today’s advances in surgery, diagnostics, and disease management are designed to deliver results that stay reliable for years, not just weeks after a procedure.
When you look at the advancements in eye care procedures enhancing long-term visual clarity, a few stand out. Refractive options like LASIK and SMILE have become more precise, with faster recovery and more predictable outcomes. Cataract surgery has evolved, too, with premium IOL implants that can improve clarity and expand your range of focus. For glaucoma, minimally invasive glaucoma surgery (MIGS) offers pressure control with less disruption. And tools like optical coherence tomography (OCT) help doctors catch changes earlier and track them more accurately over time.
The big shift is simple: more stability, fewer repeat fixes.
Which Eye Care Advances Matter Most Now?
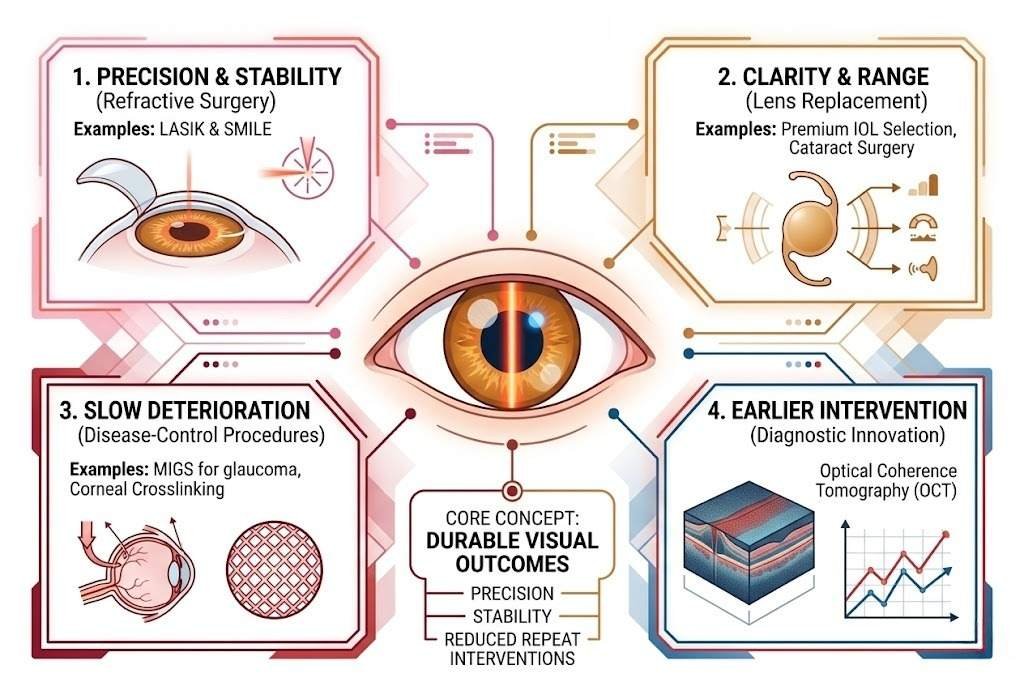
Modern eye care progress falls into four broad categories, each contributing to durable visual outcomes in a distinct way. Refractive surgery, including LASIK and SMILE, has become more precise and more stable over time. Lens replacement through cataract surgery, now guided by premium IOL selection, addresses both clarity and functional range. Disease-control procedures like MIGS for glaucoma and corneal crosslinking for keratoconus focus on slowing deterioration rather than simply sharpening sight. Underpinning all of these is diagnostic innovation, particularly optical coherence tomography, which has made earlier and more accurate intervention possible across nearly every area of eye care.
Long-term visual clarity, in this context, is not just about how well someone sees after a procedure. It is about precision, stability, and reducing the need for repeated interventions over time.
How Refractive Surgery Became More Precise
The story of modern refractive surgery is largely a story of precision. Earlier generations of procedures corrected vision, but the margin for error was wider and long-term stability was harder to predict. Advances in laser technology and surgical planning have since significantly closed that gap. For patients evaluating a reliable vision correction procedure, predictability, tissue preservation, and individual candidacy are now the key factors that distinguish one approach from another.
Laser Mapping and Wavefront-Guided Planning
The introduction of the femtosecond laser marked a turning point in how surgeons approach corneal tissue. Rather than using a mechanical blade to create the flap in LASIK, the femtosecond laser allowed for a far more controlled incision, reducing variability and improving consistency across patients with different refractive errors.
Wavefront-guided planning added another layer of individualization. By mapping the unique optical imperfections of each eye, rather than relying on a standardized prescription, surgeons could address irregularities beyond simple myopia or astigmatism. This level of customization translates directly into sharper visual acuity outcomes and fewer complaints of post-surgical night vision disturbances.
Why SMILE and Modern LASIK Hold Up Better
The comparison between SMILE and LASIK has become more nuanced as long-term data have emerged. SMILE involves extracting a small disc of tissue through a minimal incision without creating a corneal flap, which results in less disruption of the anterior corneal nerves and a more structurally intact cornea after the procedure.
Five-year SMILE refractive surgery outcomes suggest that visual acuity stability remains high over time, with low regression rates in appropriately selected patients. Modern LASIK, especially when guided by wavefront mapping, also demonstrates strong durability, making each approach well-suited to different patient profiles depending on corneal thickness, prescription range, and individual anatomy.
For patients whose corneas are too thin or whose prescriptions fall outside the treatable range for laser reshaping, the Implantable Collamer Lens offers an alternative path to long-term clarity without permanently altering corneal tissue.
New Lens Implants Expand Clear Vision Range
Cataract surgery has traditionally been understood as a procedure to remove a clouded lens and restore basic sight. Over the past decade, however, the goals have expanded considerably, with surgeons now approaching lens replacement as an opportunity to address refractive error and simultaneously reduce dependence on glasses.
What Premium IOL Designs Change After Cataracts
The shift toward refractive precision in cataract surgery centers on the intraocular lens selected to replace the natural one. Standard monofocal lenses restore clarity at a single fixed distance, typically distance vision, leaving patients to rely on reading glasses for near tasks. Premium IOL designs have moved beyond that limitation.
Trifocal IOL technology distributes light across three focal points, near, intermediate, and far, allowing patients to shift between visual tasks without constantly reaching for glasses. Extended-depth-of-focus lenses take a different approach, creating a continuous, elongated focal range rather than distinct zones, which tends to produce smoother transitions between distances.
The tradeoff worth understanding is contrast sensitivity. Trifocal designs split incoming light to cover multiple distances, and for some patients, this reduces contrast in low-light environments or introduces mild halos around light sources at night. Surgeons typically weigh a patient’s visual priorities, such as how much time they spend driving at night versus reading, before recommending one design over another.
Spectacle independence is a realistic outcome for many patients after premium cataract surgery, though the degree varies. Selecting the right intraocular lens design is what makes the difference between simply restoring vision and sustaining functional clarity across the full range of daily tasks for years after the procedure.
Procedures That Slow Vision Loss Over Time
Not every advancement in eye care is about sharpening what someone can see today. Some of the most meaningful progress has come from procedures designed to slow or halt the progression of conditions that, left unmanaged, gradually erode visual function.
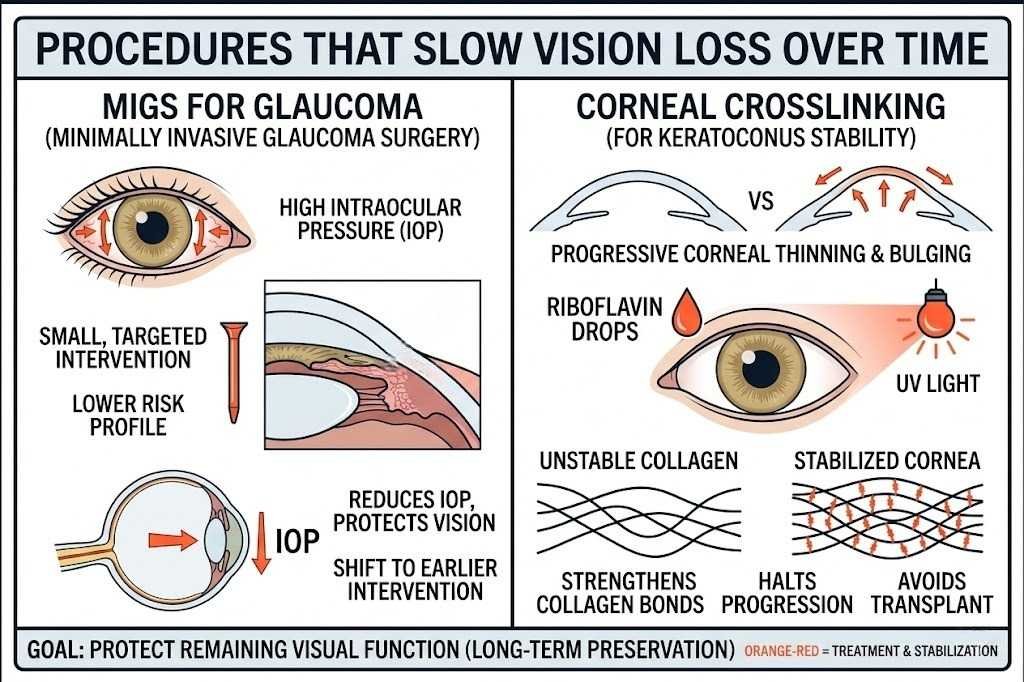
MIGS for Glaucoma with Less Tissue Disruption
Glaucoma damages the optic nerve due to elevated intraocular pressure, and managing that pressure consistently is central to preserving vision. Traditional surgical options worked, but they involved significant tissue disruption and recovery time that made them difficult to justify in earlier disease stages.
Minimally invasive glaucoma surgery, or MIGS, changed that calculation. These procedures reduce intraocular pressure through small, targeted interventions that preserve surrounding tissue and carry a lower risk profile than conventional surgery. Because MIGS can be performed at the same time as cataract surgery, many patients receive pressure management and lens replacement in a single procedure, making it practical to address glaucoma earlier, before pressure-related damage has had years to accumulate.
The goal is not to restore what has been lost but to protect what remains. In that sense, MIGS represents a shift toward earlier, lower-burden intervention as a long-term preservation strategy.
Corneal Crosslinking for Keratoconus Stability
Keratoconus causes the cornea to progressively thin and bulge, distorting vision and making it harder to manage over time. The condition tends to worsen through young adulthood, and without intervention, patients may eventually require a corneal transplant.
Corneal crosslinking uses riboflavin eye drops combined with ultraviolet light to strengthen the collagen bonds within corneal tissue. The procedure does not reverse existing distortion, but it halts progression by making the cornea structurally more resistant to further change. That distinction matters because corneal crosslinking is a disease-modifying intervention rather than a corrective one, and its value lies entirely in what it prevents. For younger patients caught early, stabilizing the cornea preserves their long-term options for visual correction in ways that would otherwise be foreclosed by continued deterioration.
Why Diagnosis Now Shapes Better Outcomes
The ability to intervene at the right moment depends heavily on what clinicians can detect and how clearly they can see it. Advances in diagnostic technology have significantly shifted that standard, enabling identification of structural changes well before symptoms become noticeable.
Optical coherence tomography plays a central role in this shift. By producing high-resolution cross-sectional images of retinal tissue, it allows clinicians to detect subtle changes in layer thickness or structure that earlier imaging methods would have missed entirely. This level of detail supports earlier decisions about when to act and how.
Artificial intelligence has added meaningful capacity on top of that imaging foundation. AI-assisted analysis helps interpret scan data at scale, flag patterns that warrant closer attention, and support risk stratification across large patient populations. In conditions like diabetic retinopathy, where progression can be slow and subtle until it isn’t, that kind of systematic review makes a measurable difference in how many patients are identified at a stage when vision preservation is still possible.
For those looking for trusted eye care resources and tips, understanding these diagnostic tools is a useful starting point. Earlier detection, more accurate planning, and better-matched treatment timing are what translate diagnostic precision into long-term visual outcomes.
Other Advances Changing Long-Term Eye Care
Beyond the established procedural categories covered so far, a few emerging areas are reshaping what long-term eye care can achieve. These advances are still developing, but they are already influencing how specialists approach preservation and treatment frequency in patients with chronic or inherited conditions.
Gene Therapy and Sustained Treatment Delivery
Gene therapy is one of the most significant emerging approaches to treating inherited retinal disease. For conditions caused by specific genetic mutations, such as certain forms of congenital blindness, gene therapy introduces a functional copy of the defective gene directly into retinal cells, addressing the underlying cause rather than managing symptoms. Early clinical results have been promising enough to shape specialists’ thinking about preservation in patients who previously had very limited options.
Sustained drug delivery addresses a different but equally important challenge: reducing the frequency of treatment for patients with chronic eye conditions. Rather than requiring frequent injections to manage diseases like wet age-related macular degeneration, sustained-release implants and extended-acting formulations can maintain therapeutic drug levels over months. This reduces treatment burden while helping maintain consistent control of disease progression.
Frequently Asked Questions
What is the difference between LASIK and SMILE?
- Both procedures correct refractive errors by reshaping the cornea, but SMILE does so without creating a corneal flap. This leaves the corneal structure more intact and may reduce post-operative dryness for some patients.
Can premium IOLs fully eliminate the need for glasses?
- Many patients achieve significant spectacle independence after premium lens implantation, though outcomes vary based on the IOL design chosen and individual visual demands. Some patients may still need glasses for specific tasks.
At what stage is corneal crosslinking recommended?
- It is typically recommended when keratoconus is detected early and still progressing, as the procedure halts deterioration rather than reversing existing distortion.
Is gene therapy currently available for inherited retinal disease?
- Approved options exist for specific genetic mutations, though the field is still expanding, and eligibility depends on the underlying condition and its genetic profile.
What Long-Term Visual Clarity Depends On
Lasting visual clarity rarely comes from a single procedure. It depends on matching the right intervention to the right condition, understanding how individual eye anatomy shapes outcomes, and maintaining diagnostic follow-up to catch changes before they compound.
The procedures covered here, from refractive surgery and premium intraocular lens implants to MIGS and corneal crosslinking, each address a distinct aspect of visual function. Taken together, they reflect a framework built around correction, preservation, and durability rather than short-term fixes.
Visual acuity over time is also shaped by habits that support eye health beyond the clinic, including protecting your eyes from UV damage, which remains one of the more consistently overlooked factors in long-term eye care.
Disclaimer
The information provided in this article is for educational and informational purposes only and should not be considered medical advice, diagnosis, or treatment. Eye care procedures, outcomes, and suitability vary significantly based on individual health conditions, eye anatomy, and professional evaluation. Always consult a qualified ophthalmologist or eye care specialist before making decisions about surgical or non-surgical treatments. The authors and publishers are not responsible for any actions taken based on this content.
References
- Ang, M., et al. (2019). Small incision lenticule extraction (SMILE) versus LASIK: a systematic review and meta-analysis. DOI: https://doi.org/10.1016/j.survophthal.2019.01.006
- Kohnen, T., et al. (2020). Multifocal intraocular lenses: an update on clinical outcomes and patient satisfaction. DOI: https://doi.org/10.1016/j.jcrs.2020.02.031
- Saheb, H., & Ahmed, I. I. K. (2012). Micro-invasive glaucoma surgery: current perspectives and future directions. DOI: https://doi.org/10.1016/j.survophthal.2012.02.001
- Raiskup, F., & Spoerl, E. (2013). Corneal crosslinking with riboflavin and ultraviolet A. Part II. Clinical indications and results. DOI: https://doi.org/10.1007/s00347-013-2872-7
- Huang, D., et al. (1991). Optical coherence tomography. DOI: https://doi.org/10.1126/science.1957169
- Campochiaro, P. A. (2018). Gene transfer for retinal disease: progress and perspectives. DOI: https://doi.org/10.1016/j.ophtha.2017.12.024
- Holekamp, N. M. (2021). Review of sustained-release drug delivery for retinal diseases. DOI: https://doi.org/10.1016/j.ophtha.2020.09.040