
Many practice owners assume that clinical excellence and patient volume are enough to guarantee financial health. The reality is far more complicated. A practice can deliver outstanding care, attract a steady stream of patients, and still struggle to meet payroll if its revenue cycle is broken. Taking proactive steps to strengthen this foundation empowers staff and creates real control over the practice’s financial future.
Walk into any successful women’s health practice, and you will see the visible signs of success: full waiting rooms, engaged clinicians, satisfied patients, and a team that moves with purpose. What you will not see is the financial machinery operating quietly in the background, processing claims, chasing denials, verifying coverage, and collecting payments. Yet this invisible system determines whether a practice thrives, survives, or slowly drains its own resources.
Disconnect Between Clinical Success and Financial Performance

Why Busy Practices Still Struggle Financially
It is one of the most frustrating paradoxes in healthcare. A practice can be fully booked for weeks, employ skilled providers, and maintain glowing patient reviews, yet still face cash flow problems month after month. The cause is rarely a lack of demand. It is almost always a breakdown somewhere in the financial process that turns clinical work into collected revenue.
Obstetrics and gynecology present some of the most complex billing challenges in all of medicine. The global maternity package alone requires practices to track months of antepartum visits before any reimbursement is released. Add multi-procedure surgeries, evaluation and management overlaps, and constantly shifting payer rules, and you have a recipe for revenue leakage that volume alone cannot fix. Recognizing these complexities helps practices feel understood and better prepared to address them.
True Cost of Inefficient Financial Operations
When financial operations falter, the damage shows up in measurable ways. Days in accounts receivable creep upward net collection ratios slip. Denials pile up faster than staff can work them. The patient’s age exceeds the point where most can be collected.
Healthy practices typically maintain a clean claims rate above 95 percent and keep days in accounts receivable below 35 days. When these benchmarks slip by even a few percentage points, the financial impact compounds quickly. A practice that collects 88 percent of its legitimately owed revenue, rather than 96 percent, is effectively giving away the equivalent of one full provider’s salary every year.
What a Revenue Cycle Actually Looks Like in Women’s Health
Complete Patient-to-Payment Journey
The revenue cycle begins long before a claim is ever submitted and ends long after a service is rendered. It starts when a patient calls to schedule an appointment and continues through insurance verification, the clinical visit itself, charge capture, coding, claim submission, payment posting, denial management, and finally patient balance collection.
Each stage hands off to the next, and every handoff is a potential failure point. A misspelled name in scheduling can result in a denial six weeks later. An overlooked modifier during coding can reduce a payment by hundreds of dollars. A missed authorization can turn an otherwise valid claim into a write-off.
Why OB/GYN Differs From Other Specialties
Women’s health practices face billing complexities that few other specialties encounter. The table below illustrates how OB/GYN coding diverges from typical specialty billing.
| Billing Element | General Specialty Billing | OB/GYN Billing |
|---|---|---|
| Service Span | Single encounter | Up to 10 months for maternity care |
| Bundling Rules | Standard, less complex | Requires a global obstetric package |
| Common Modifiers | Limited use | Frequent use of 22, 25, 51, 59 |
| Procedure Overlap | Rare | Common in surgical sessions |
| Authorization Complexity | Moderate | High, especially for high-risk care |
| Documentation Volume | Standard | Significantly higher |
| Payer-Specific Rules | Manageable | Extensive variation |
This is precisely why specialized obgyn medical billing services consistently outperform generalist billing teams. The depth of knowledge required to handle the global maternity package, manage modifier 22 for unusually difficult deliveries, and correctly bill for procedures performed during an annual exam cannot be picked up on the job.
Common Failure Points That Drain Revenue
Eligibility Verification Gaps
A surprising number of denials trace back to a single moment at the front desk. When eligibility is not verified in real time or when benefit details are misinterpreted, the resulting claim is built on a faulty foundation. Weeks later, the denial arrives, and staff must scramble to recover information that was readily available at the time of service.
Coding Errors and Missed Charges
Coding mistakes go in both directions. Undercoding leaves money on the table. Overcoding creates compliance risk. Both undermine the practice’s long-term financial health.
Common problem areas in women’s health include incorrect application of the global maternity package when patients change providers mid-pregnancy, improper use of modifier 25 for separately identifiable evaluation services performed alongside a procedure, and missed billing for items such as IUD insertions during routine visits.
Denial Management Neglect
Many practices treat denials as a cost of doing business rather than recoverable revenue. Yet industry data consistently shows that roughly two-thirds of denied claims are recoverable, and nearly 90 percent are preventable when root causes are identified and addressed.
The problem is rarely a lack of willingness. It is a lack of time and expertise. Working denials properly requires specialized knowledge of payer rules, appeal procedures, and documentation standards that most in-house teams cannot maintain alongside their daily responsibilities.
Slow or Inconsistent Patient Collections
With high-deductible health plans now the norm, patient responsibility represents a growing share of total practice revenue. Estimates suggest that patient payments now account for 30 percent or more of total collections at many women’s health practices. Yet patient balances remain one of the most poorly managed revenue streams in the industry.
Unclear statements, the lack of payment plan options, and inconsistent follow-up leave substantial money uncollected. Modern practices recognize that patient-pay revenue requires the same discipline as insurance reimbursement.
Human and Operational Costs of a Broken Revenue Cycle
Financial dysfunction does not stay confined to the billing department. It spreads through every layer of the practice. Front desk staff who spend their afternoons fighting denials cannot welcome patients with the warmth a women’s health practice depends on. In-house billers who feel they are losing ground every week eventually leave, taking their institutional knowledge with them. Physicians who are pulled into documentation queries and coding clarifications lose the focused energy their patients deserve.
A practice operating at the edge of its administrative capacity also cannot grow. Adding a new provider requires bandwidth that does not exist. Expanding into ultrasound, in-office procedures, or telehealth becomes impossible when the existing operation is already overwhelmed. The financial strain quietly caps the practice’s potential.
Building a Healthier Revenue Cycle
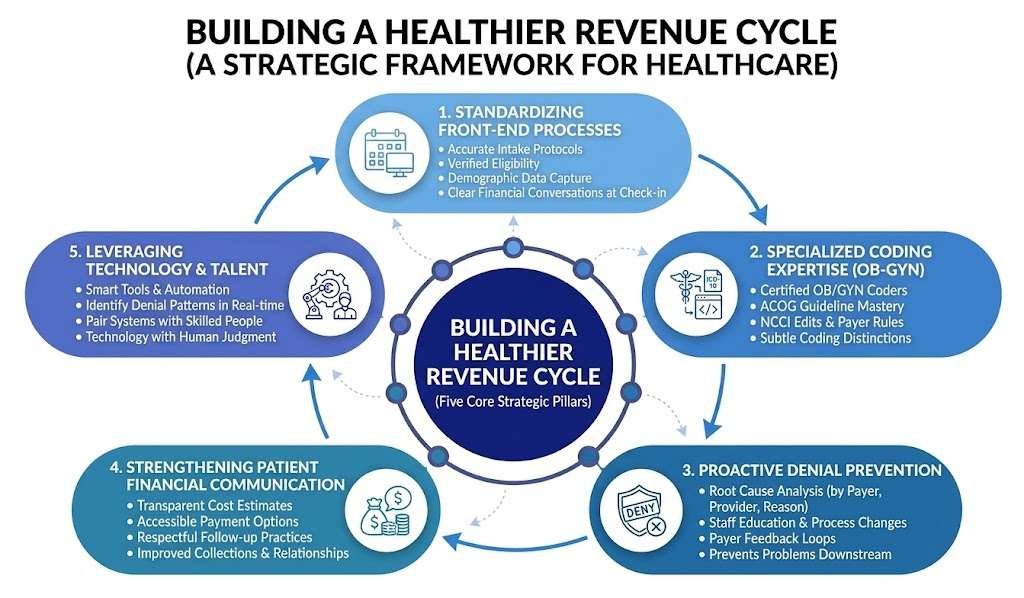
Standardizing Front-End Processes
The strongest revenue cycles begin before the patient ever sees the provider. Standardized intake protocols, verified eligibility, accurate demographic data capture, and clear financial conversations at check-in prevent most downstream problems. When the front desk operates with discipline, the rest of the cycle follows naturally.
Investing in Specialized Coding Expertise
Generalist coders rarely have the depth required for accurate coding in women’s health. Certified coders who specialize in obstetrics and gynecology understand ACOG guidelines, National Correct Coding Initiative edits, payer-specific rules, and the subtle distinctions that separate a clean claim from a denial. This specialization is not a luxury. It is the difference between collecting what you earn and watching it disappear.
Implementing Proactive Denial Prevention
Reactive denial management is exhausting and expensive. Proactive denial prevention is sustainable and profitable. Leading practices analyze denial patterns by payer, provider, and reason, then address root causes through staff education, process changes, and payer feedback loops. The goal is not to work on denials faster but to prevent them from occurring in the first place.
Strengthening Patient Financial Communication
Transparent cost estimates, accessible payment options, and respectful follow-up practices improve both collections and patient relationships. Patients who understand what they owe and have reasonable ways to pay are far more likely to settle their balances than patients who receive confusing statements weeks after their visit.
Leveraging Technology Without Overrelying on It
Modern revenue cycle platforms can automate eligibility checks, flag coding inconsistencies before submission, and identify denial patterns in real time. But technology alone is not a strategy. The practices that get the most from their systems are the ones that pair smart tools with skilled people. Software cannot replace the judgment of an experienced coder, but it can multiply that coder’s effectiveness across thousands of claims.
When to Consider Outside Support
Signs Your In-House Operations Have Reached Their Limit
Honest self-assessment is difficult but essential. Practices should consider outside support when they notice rising days in accounts receivable, increasing denial rates, frequent turnover in billing roles, missed filing deadlines, or a persistent feeling that financial reporting raises more questions than it answers. These are not failures of effort. There are signs that the operation has outgrown its current structure.
What Specialized Partners Bring to the Table
Specialized OB/GYN billing services offer capabilities that most in-house teams cannot match. These include certified women’s health coders, dedicated denial management teams, advanced analytics, scalable capacity, transparent reporting, and the institutional knowledge that comes from working exclusively with obstetric and gynecologic claims. The goal of the partnership is not to replace the internal team but to extend its capabilities.
Choosing the Right Partner
Not every billing company is equipped for women’s health. Practices evaluating potential partners should look for demonstrated experience in obstetrics and gynecology, transparent performance metrics, certified coding staff, strong compliance practices, and clear communication protocols. The best partnerships are built on alignment of values, not just price.
A Real-World Improvement Example
An illustrative case helps frame what is possible. A mid-sized OB/GYN group in the Midwest saw its days in accounts receivable rise from 38 to 56 over eighteen months. After partnering with a specialized billing team, the practice reduced AR days to 31 within six months, recovered more than $180,000 in previously written-off claims, and increased its net collection ratio from 89 percent to 96 percent. The improvement came not from a single change but from the disciplined application of specialized expertise across the entire revenue cycle. (Note: this example is illustrative.)
Key Performance Benchmarks Worth Tracking Monthly
A healthy revenue cycle is measurable. The metrics below give practice owners a clear view of where things stand and where attention is needed.
| Metric | Healthy Range | Warning Sign |
|---|---|---|
| Clean Claims Rate | 95% or higher | Below 90% |
| Days in Accounts Receivable | Under 35 days | Over 45 days |
| Net Collection Ratio | 95% or higher | Below 90% |
| Initial Denial Rate | Under 5% | Over 10% |
| Patient Collection Rate | Above 70% | Below 50% |
| AR Over 90 Days | Under 15% | Over 25% |
Reviewing these numbers monthly, rather than quarterly, allows practices to catch drift before it becomes a crisis.
Frequently Asked Questions
How long does it take to see improvement after fixing revenue cycle issues?
- Most practices see early improvements in clean claim rates within 30 to 60 days. Full benefits, including AR reduction and net collection improvements, typically materialize over three to six months.
Should small OB/GYN practices outsource billing entirely?
- Not necessarily. Some small practices do well with hybrid models, retaining front-desk and patient communication functions in-house while outsourcing coding and denial management. The right structure depends on volume, complexity, and internal capacity.
What is the single most overlooked failure point in OB/GYN billing?
- Modifier usage. Misapplied or missing modifiers, particularly 22, 25, and 59, account for a significant share of preventable denials in women’s health.
How much does a broken revenue cycle actually cost a practice?
- Industry analyses suggest that practices with weak revenue cycles lose between 5 and 15 percent of legitimately earned revenue annually. For a practice grossing $2 million, that translates to a loss of $100,000 to $300,000 in income each year.
What are the most common reasons claims get denied in women’s health?
- Top causes include eligibility issues, missing or incorrect modifiers, lack of authorization, documentation gaps for medical necessity, and incorrect application of the global maternity package.
Long-Term Vision of a Healthy Practice
A healthy revenue cycle is not in tension with patient care. It is the foundation that makes excellent care sustainable. A practice that collects what it earns can invest in better equipment, attract stronger talent, expand its services, and serve patients with greater consistency over time.
Practices with disciplined financial operations also weather change far better than those operating on fragile cash flow. Payer rules shift. Regulations change. Economic pressures rise and fall. The practices that endure are the ones that built financial resilience into their daily operations long before they needed it.
Conclusion
Behind every thriving women’s health practice is a quietly excellent financial operation that patients never see and that even many practice owners underestimate. Clinical excellence is essential, but it is not sufficient on its own. The practices that flourish over decades recognize financial health and clinical health as inseparable.
The journey toward a healthier revenue cycle is rarely a single fix. It is the disciplined, ongoing work of building specialized, continuously improving processes from the front desk to the final patient payment. Whether the path forward involves internal improvements, smarter technology, or partnership with a specialized team, the first step is the same: an honest look at the numbers, an honest assessment of what they reveal, and the willingness to act on what you find.
Your patients trust you with their care. The question worth asking is whether your revenue cycle deserves the same level of trust.
Disclaimer
This article is for informational purposes only and does not constitute medical, legal, financial, or billing advice. It is not a substitute for consultation with qualified professionals such as licensed healthcare administrators, CPCs, or revenue cycle specialists.
Data and benchmarks are based on publicly available sources and may vary depending on factors like practice size, specialty, location, and staffing. No outcomes are guaranteed, and the included case study is illustrative only.
References to organizations or vendors are for information, not endorsement. Regulations, coding standards, and payer rules may change, so readers should verify details with authoritative sources (e.g., CMS, ACOG, HFMA).
This article was created with editorial assistance and should be reviewed by a qualified expert before formal use.
References
- Chandawarkar R, Nadkarni P, Barmash E, Thomas S, Capek A, Casey K, Carradero F. Revenue Cycle Management: The Art and the Science. Plastic and Reconstructive Surgery, Global Open. 2024 Jul 2; 12(7): e5756. DOI: 10.1097.GOX.0000000000005756. Available at: pmc.ncbi.nlm.nih.gov/articles/PMC11219169
- Alradhi Z, Alanazi A. The Road Ahead and Challenges of Revenue Cycle Management in Saudi Governmental Hospitals. Healthcare (Basel). 2023 Oct 12; 11(20): 2716. DOI: 10.3390/healthcare11202716. Available at: mdpi.com.2227-9032.11.20.2716
- Bhagavath B, Goodman L, Petrozza J. Billing, Coding, and Practice Management: A Primer for Today’s Reproductive Medicine Professional. Fertility and Sterility. 2021 Jan; 115(1): 22-28. DOI: 10.1016/j.fertnstert.2020.11.023.
- Ouillette R, Wessel L. Revenue Cycle Management, Hand Surgery Specialty Focus. Hand Clinics. 2024 Nov; 40(4): 459-466. DOI: 10.1016/j.hcl.2024.05.003.
- Healthcare Financial Management Association (HFMA). Claim Integrity Task Force: Standardizing Denial Metrics for Revenue Cycle Benchmarking and Process Improvement. 2022. Available at: hfma.org.guidance.standardizing-denial-metrics-revenue-cycle-benchmarking-process-improvement
- Healthcare Financial Management Association (HFMA). Redesigning Denials Management in the OBBBA Era. 2025. Available at: hfma.org.revenue-cycle.redesigning-denials-management-in-the-obbba-era
- Medical Group Management Association (MGMA). Benchmarking Report on Denials and Appeals. 2024. Available at: mgma.com (full report via MGMA membership).
- Healthcare Financial Management Association (HFMA), referenced in MD Clarity. Patient Financial Responsibility. 2024. Available at: mdclarity.com/blog/patient-financial-responsibility
- My Medical Bill Solution. OB/GYN Revenue Cycle: KPIs and Benchmarks. 2025. Available at: mymedicalbillsolution.com.billing.ob-gyn.revenue-cycle
- Contemporary OB/GYN. Get a Grip on Revenue Cycle Management. 2025. Available at: contemporaryobgyn.net. view. get-a-grip-on-revenue-cycle-management
- American College of Obstetricians and Gynecologists (ACOG). Payment in Practice: 2025 OB/GYN Coding Manual. 2025. Available at: acog.org.store.products.coding-resources.payment-in-practice-2025-obgyn-coding-manual
- RAND Corporation. Analysis of High-Deductible Health Plans. Keeler E, Manning W, Newhouse J, et al. RAND Health Insurance Experiment series. Available at: rand.org.pubs.technical_reports.TR562z4
- RevGen Billing. Patient Responsibility and High-Deductible Plans: Billing Strategies to Reduce Bad Debt. 2026. Available at: revgenbilling.com.patient-responsibility-high-deductible-plans