
According to the North American Spine Society‘s 2023 research data, between 10 and 40 percent of back surgeries result in persistent or worsening symptoms, a condition known as Failed Back Surgery Syndrome. As spinal procedures become increasingly sophisticated, this persistent failure rate highlights a critical challenge. Many patients struggle to distinguish between normal postoperative discomfort and signs that their surgery has actually failed to address the underlying problem.
The stakes of missing these warning signs extend far beyond continued pain. While typical surgical recovery follows predictable patterns, failed back surgery creates a complex web of symptoms that can worsen without proper intervention. Scar tissue formation, nerve damage, and hardware complications can transform what should be a healing process into a cycle of escalating dysfunction. For the thousands of Americans navigating post-surgical recovery each year, understanding when a revision spinal procedure in New Jersey may be necessary becomes essential for protecting both immediate comfort and long-term spinal health.
What makes recognition particularly challenging is that failed surgery symptoms often mimic normal recovery phases, creating confusion about when to seek help versus when to wait for natural healing. The following analysis breaks down the specific warning signs, underlying mechanisms, and diagnostic approaches that separate surgical success from failure.
How to Tell Failed Back Surgery Symptoms from Normal Postoperative Pain
Recovery Timeline and Pain Progression
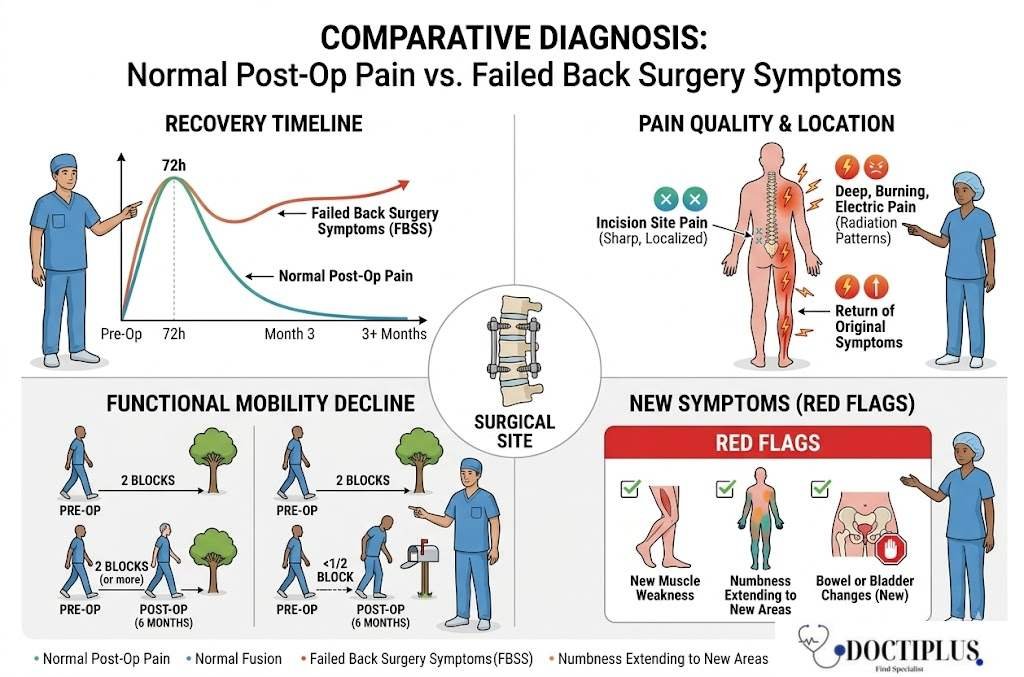
The timeline tells the first part of the story. Normal postoperative pain follows a predictable pattern. It peaks within the first 72 hours, then gradually decreases over 6 to 12 weeks. Failed back surgery symptoms, by contrast, either plateau without improvement after the initial healing period or actually worsen as weeks pass. When pain levels remain consistently high three months after surgery, or when they improve initially but then return with equal or greater intensity, these patterns signal potential surgical failure rather than extended recovery.
Pain Location, Quality, and Radiation Patterns
Location and quality of pain provide equally important clues. Surgical site pain from incisions typically feels sharp and localized, improving as tissues heal. Failed surgery pain often presents as deep, burning, or electric sensations that radiate beyond the surgical area. Many patients describe a return of their original symptoms, the exact pain patterns that led them to surgery in the first place. This recurrence, especially when combined with new areas of discomfort, strongly suggests the underlying spinal problem remains unresolved.
Functional Decline After Initial Improvement
Functional limitations offer another critical distinction. Normal recovery involves gradual improvement in mobility, even if progress feels slow. Failed surgery maintains or worsens pre-surgical limitations. Consider someone who could walk two blocks before surgery but struggles to walk to the mailbox six months afterward. Or someone whose leg numbness was supposed to resolve but has actually spread to new areas. These functional declines, particularly when they occur after an initial improvement period, indicate that the surgery has not achieved its intended goals.
New Symptoms That Were Not Present Before Surgery
New symptom emergence marks the clearest red flag. Weakness in previously unaffected muscles, numbness extending to new body areas, or bowel and bladder changes that were not present before surgery all suggest complications beyond normal healing. When patients develop symptoms they never experienced pre-surgically, the body is often signaling that something has gone wrong with either the healing process or the surgical intervention itself.
- Pain that plateaus or worsens three months after surgery.
- Return of the original pre-surgery pain pattern.
- Burning, electric, or shooting sensations in the legs.
- New weakness or numbness in previously healthy areas.
- Bowel or bladder changes that did not exist before the procedure.
What Causes Symptoms After Back Surgery to Persist or Worsen
Understanding why symptoms continue requires examining both biological and mechanical factors that can undermine surgical success. The spine’s complex anatomy means that even technically successful procedures can fail to address all sources of pain, while healing complications can create entirely new problems. These underlying mechanisms help explain why some patients experience continued suffering despite following all post-surgical protocols.
How Scar Tissue and Nerve Damage Affect Recovery
Scar tissue formation represents one of the most common yet underappreciated causes of persistent symptoms. Every surgical procedure triggers the body’s natural healing response, which includes collagen production and tissue repair. In the spine, however, this scar tissue can form around nerve roots and in the epidural space, essentially creating new sources of compression and irritation. What begins as protective healing can turn into a mechanical problem when scar tissue adheres to nerve structures, limiting their normal movement and causing chronic inflammation.
The symptoms of scar tissue-related complications often differ from those of the original problem. Instead of the sharp, localized pain that might have prompted surgery, patients frequently report burning, aching sensations that seem to wrap around their back and into their legs. This epidural fibrosis can develop months after surgery, explaining why some patients feel better initially but then experience symptom return as scar tissue matures and contracts.
Nerve damage during surgery, while relatively uncommon, creates its own distinct symptom profile. Neuropathic pain, the burning, electric, shooting sensations that result from nerve injury, often proves more challenging to treat than the original mechanical compression. Patients describe these sensations as fundamentally different from any pain they experienced before surgery. The damaged nerves misfire, sending pain signals even when no actual tissue damage is occurring. This explains why traditional pain medications often prove ineffective for post-surgical neuropathic symptoms.
Hardware Failure and Spinal Instability as Symptom Sources
Spinal fusion procedures rely on hardware like rods, screws, and plates to maintain proper alignment while bone grows together. When this hardware loosens, breaks, or shifts position, it creates both mechanical instability and localized irritation. Unlike scar tissue problems that develop gradually, hardware failure often announces itself with sudden changes in symptom patterns. Patients might experience sharp pain with specific movements, clicking or grinding sensations, or a return of the mechanical back pain that surgery was meant to eliminate.
Pseudoarthrosis, the failure of bones to fuse properly, creates ongoing instability that undermines the entire surgical goal. When vertebrae do not fuse as intended, they continue to move independently, generating inflammation and mechanical stress. This ongoing motion prevents proper healing and often recreates the exact conditions that necessitated surgery in the first place. The symptoms typically worsen with activity and may improve with rest, mimicking the pre-surgical pattern many patients hoped to escape forever.
Spinal instability, whether from hardware problems or fusion failure, also affects surrounding structures. Muscles work overtime trying to compensate for mechanical weakness, leading to chronic tension and fatigue. Adjacent vertebrae may experience increased stress, potentially accelerating degenerative changes that create new sources of pain. This cascade effect explains why some patients develop symptoms in spinal areas that were not part of their original problem.
How Doctors Diagnose Failed Back Surgery Syndrome
Clinical History and Symptom Mapping
Diagnosing failed back surgery requires distinguishing between multiple potential causes of persistent symptoms. The process begins with a detailed clinical history that maps symptom patterns against the surgical timeline. Physicians particularly focus on when symptoms began relative to surgery, how they have changed over time, and whether they match the original complaint or represent new problems. This temporal relationship often provides the first clue about whether symptoms stem from incomplete healing, surgical complications, or entirely new spinal issues.
Physical and Neurological Examination
Physical examination reveals functional changes that imaging might miss. Doctors assess range of motion, muscle strength, and neurological responses to determine whether the surgery achieved its intended goals. A straight leg raise test that remains positive months after disc surgery, or new muscle weakness in areas that should have improved, suggests ongoing nerve compression or damage. These clinical findings help physicians understand not just whether symptoms persist, but why they persist.
Advanced Imaging and MRI Interpretation
Magnetic Resonance Imaging (MRI) serves as the primary diagnostic tool for evaluating post-surgical anatomy. Advanced MRI sequences can distinguish between scar tissue and disc material, assess fusion progress, and identify hardware positioning problems. However, interpreting post-surgical MRI requires specialized expertise, as normal healing changes can mimic pathological findings. Gadolinium-enhanced imaging helps differentiate recurrent disc herniations from epidural scarring, a distinction that significantly affects treatment decisions.
Electrodiagnostic Testing for Nerve Function
Electrodiagnostic studies, including nerve conduction velocity tests and electromyography, help identify specific nerve damage that may not be apparent on imaging. These tests measure how well nerves conduct electrical signals and whether muscles receive proper nerve input. When a patient reports persistent numbness or weakness, these studies can pinpoint whether the problem stems from ongoing compression, surgical nerve damage, or incomplete nerve recovery. For patients considering a revision spinal procedure in New Jersey, these diagnostic findings help surgeons understand exactly what went wrong and plan more targeted interventions.
Why Managing Persistent Symptoms After Back Surgery Is Challenging
Limits of Traditional Pain Medication
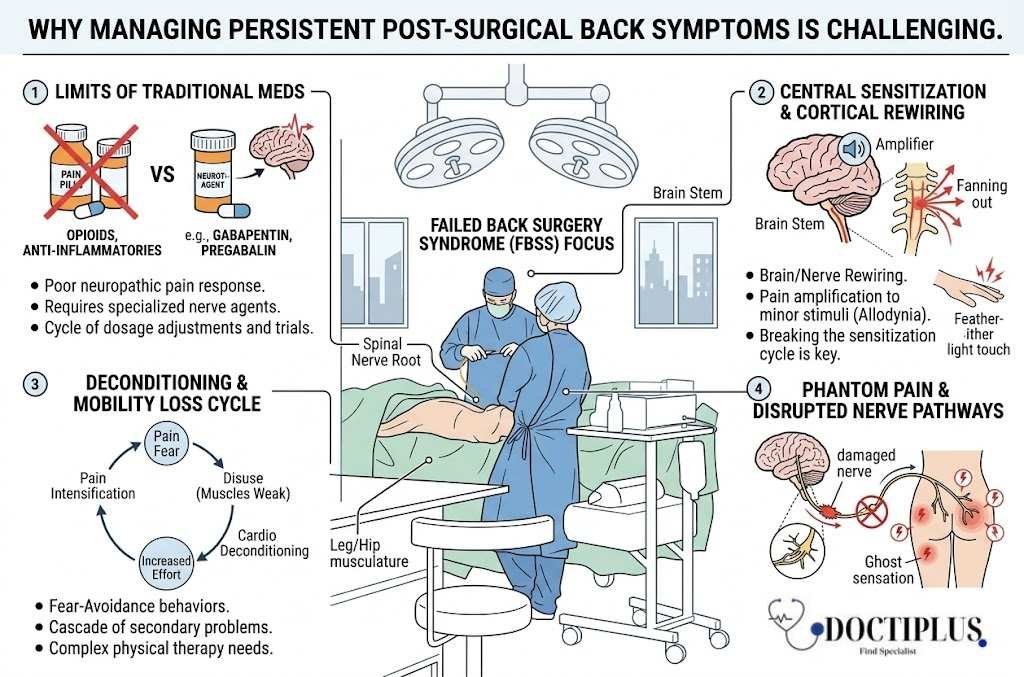
Failed back surgery creates a perfect storm of treatment complications that make symptom management far more complex than addressing the original spinal problem. Neuropathic pain from nerve damage responds poorly to traditional pain medications, requiring specialized drugs like gabapentin or pregabalin that work on nerve firing patterns rather than inflammation. Many patients find that medications that once provided relief no longer work, forcing them into a frustrating cycle of drug trials and dosage adjustments.
Central Sensitization and Chronic Pain Amplification
Central sensitization, where the nervous system becomes hypersensitive to pain signals, often develops in chronic post-surgical cases. The brain learns to amplify pain responses, making even minor stimuli feel intensely painful. This neurological rewiring explains why some patients experience severe pain from light touch or movement that should not cause discomfort. Breaking this sensitization cycle requires multidisciplinary approaches that address both physical and neurological aspects of pain processing.
Mobility Loss and Deconditioning Cycles
Mobility limitations create a cascade of secondary problems that complicate recovery. Patients who avoid movement due to pain experience muscle weakening, joint stiffness, and cardiovascular deconditioning. This disuse syndrome then makes any activity more difficult and painful, creating a cycle where fear of pain leads to inactivity, which leads to greater pain with any attempted movement. Physical therapy becomes crucial but challenging, as traditional exercises may need significant modification to accommodate post-surgical anatomy.
Phantom Pain and Disrupted Nerve Pathways
Phantom pain sensations add another layer of complexity for patients who experienced nerve damage during surgery. Similar to phantom limb pain in amputees, these patients feel pain in areas where nerve pathways have been disrupted. The brain continues to interpret signals from damaged nerves as coming from specific body regions, creating pain that feels real but does not correspond to actual tissue damage. This disconnect between sensation and reality makes treatment selection particularly challenging.
Which Symptom Signs Indicate Serious Complications Need Immediate Care
Progressive Neurological Deficits
Certain post-surgical symptoms demand urgent medical evaluation because they signal complications that can cause permanent damage if left untreated. Progressive neurological deficits, including worsening weakness, spreading numbness or loss of muscle control, suggest ongoing nerve compression or damage and require immediate intervention. Unlike the gradual improvement expected in normal recovery, these progressive symptoms indicate that something is actively harming nerve tissue.
Cauda Equina Syndrome as a Surgical Emergency
Cauda equina syndrome represents the most serious neurological emergency in post-surgical patients. New or worsening bowel and bladder control problems, saddle numbness around the genitals and anus, and severe weakness in both legs require emergency surgical intervention. This constellation of symptoms indicates compression of the nerve bundle at the base of the spinal cord, and delayed treatment can result in permanent paralysis and loss of bowel and bladder function.
Surgical Site Infection Warning Signs
Infection signs require equally urgent attention but can be subtle in post-surgical patients. Fever, increasing redness or warmth at the surgical site, unusual drainage, or a return of severe pain after initial improvement all suggest possible surgical site infection. Deep spinal infections can develop weeks or months after surgery and may spread to surrounding tissues or even the bloodstream if left untreated. The challenge lies in distinguishing infection symptoms from normal inflammatory healing responses.
Sudden Hardware Failure Symptoms
Hardware-related emergencies typically announce themselves with sudden, severe pain during movement, especially if accompanied by a popping or snapping sensation. These symptoms may indicate screw breakage, rod displacement, or sudden loss of spinal stability. While not always as immediately life-threatening as neurological emergencies, acute hardware failure can cause rapid deterioration and should prompt same-day medical evaluation to prevent further complications.
- Sudden inability to control bladder or bowel function.
- Numbness around the groin, buttocks, or inner thighs.
- Rapidly spreading weakness in one or both legs.
- Fever above 101 degrees Fahrenheit with wound drainage.
- Audible pop or snap followed by sharp new pain.
For patients experiencing any combination of these warning signs, the window for effective intervention may be measured in hours rather than days, making immediate medical attention essential for preserving long-term function and preventing permanent complications.
Final Conclusion
Failed back surgery is not a single event but a pattern that reveals itself over time through pain that will not settle, function that will not return, and new symptoms that do not fit the expected recovery arc. The patients who recover well from revision procedures tend to be those who recognize these signals early, document them clearly, and bring that information to a spine specialist rather than waiting for things to improve on their own. A pain diary, honest reporting of functional losses, and updated imaging often reveal more than a single office visit ever could.
Revision surgery is not the right answer for every case, but neither is years of escalating medication or withdrawal from normal life. The most productive path usually involves a careful diagnostic workup, a second opinion from a surgeon who did not perform the original procedure, and a treatment plan that weighs conservative options, targeted injections, neuromodulation, and revision surgery against each other. When red flag symptoms appear, especially cauda equina signs, infection, or sudden hardware failure, the question is no longer whether to seek care but how quickly. Acting early protects nerve tissue, preserves mobility, and gives patients the best chance of regaining a life that does not revolve around spinal pain.
Medical Disclaimer
The information provided in this article is intended for general educational and informational purposes only and does not substitute for professional medical advice, diagnosis, or treatment. Failed back surgery syndrome, revision spinal surgery, and post-operative complications are complex medical conditions that require individualized assessment by a qualified spine surgeon, neurologist, or pain specialist. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition, new or worsening symptoms, or treatment options. Never disregard professional medical advice or delay seeking it because of something you have read here. If you experience progressive weakness, loss of bowel or bladder control, fever with wound changes, or sudden severe spinal pain, seek emergency medical care immediately. Reliance on any information in this article is solely at your own risk.
References
- North American Spine Society. (2023). Research and Clinical Data on Outcomes After Spinal Surgery.
- Cleveland Clinic. (2024). Failed Back Surgery Syndrome (FBSS): Causes, Symptoms, and Treatment.
- National Institute of Neurological Disorders and Stroke. (2023). Peripheral Neuropathy Fact Sheet.
- American Academy of Orthopaedic Surgeons (OrthoInfo). (2023). Spinal Fusion and Pseudoarthrosis.
- Centers for Disease Control and Prevention. (2024). Surgical Site Infection (SSI) Guidelines.
- American Association of Neurological Surgeons. (2023). Cauda Equina Syndrome Patient Information.
- Radiological Society of North America (RadiologyInfo). (2024). Magnetic Resonance Imaging of the Spine.
- Mayo Clinic. (2023). Sciatica: Symptoms, Causes, and Diagnosis.
- Woolf, C. J. (2011). Central Sensitization: Implications for the Diagnosis and Treatment of Pain. PMC / NIH National Library of Medicine.
- MedlinePlus, U.S. National Library of Medicine. (2024). Gabapentin: Drug Information and Use in Neuropathic Pain.
- Journal of Spine Surgery. (2015). Epidural Fibrosis and Failed Back Surgery Syndrome: Pathophysiology and Clinical Implications.