
For decades, getting mental health care in America meant something very specific: finding a local provider, taking time off work, sitting in a waiting room, and hoping the schedule somehow lined up with real life. Millions of people could not clear all those hurdles. Today, a growing number of patients receive psychiatric care without ever leaving home, and the shift is changing what access to care really means.
Mental Health Access Problem in Plain Numbers
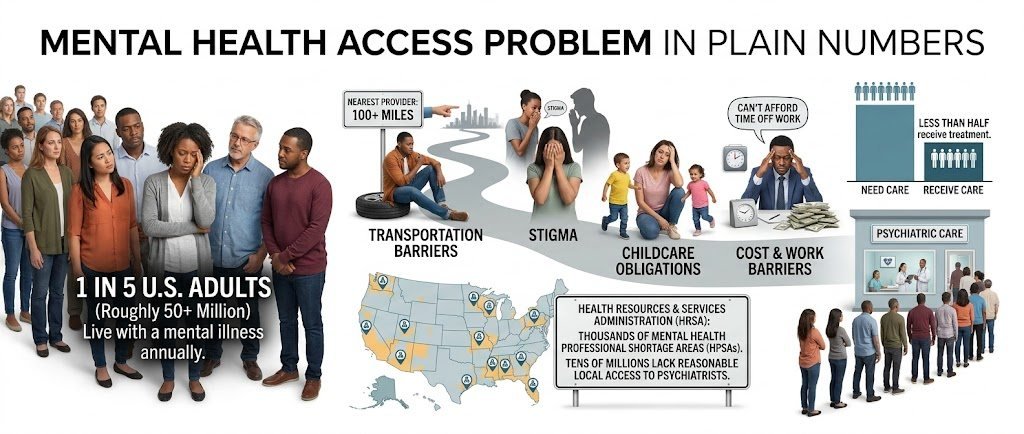
The gap between people who need behavioral health care and people who actually receive it is large. According to the National Institute of Mental Health, roughly one in five U.S. adults lives with a mental illness in any given year, yet less than half receive treatment. The shortage is even sharper for psychiatric prescribers. The Health Resources and Services Administration has designated thousands of mental health professional shortage areas, covering tens of millions of Americans who lack reasonable local access to a psychiatrist.
Add stigma, transportation barriers, childcare obligations, and the sheer cost of taking time off work, and the picture comes into focus. The issue is not always that people refuse help. Often, help is just out of reach.
What Telepsychiatry Actually Looks Like Today
Telepsychiatry is a branch of telemedicine that delivers psychiatric assessment, medication management, and therapy through secure video. A patient logs in from a phone, tablet, or computer, and a licensed clinician joins from a separate location. Sessions can happen at home, inside a primary care clinic, in a school nurse’s office, or in a correctional setting. The platform changes, but the clinical standard does not.
Most modern programs include the following:
- Initial psychiatric evaluations and diagnostic assessments
- Ongoing medication management visits
- Individual therapy with licensed counselors or social workers
- Crisis stabilization in coordination with on-site staff
- Communication and coordination with the patient’s primary care provider
The clinician you see over video has the same training, licensure, and prescribing authority as one you would meet in person. The technology is simply the bridge.
Where Telepsychiatry Is Making the Biggest Difference

Rural communities
Rural counties often have a single psychiatrist for every 30,000 residents, sometimes none at all. A small critical access hospital can now contract with remote providers and offer evaluations the same week, instead of pushing patients onto a six-month waitlist. For many rural patients, this is the first time consistent psychiatric care has ever been available without a multi-hour drive.
Correctional facilities
Jails and prisons carry a disproportionate burden of serious mental illness, with rates several times higher than the general population. Bringing psychiatrists on-site full-time is expensive and rarely sustainable. Video-based care lets a clinician see incarcerated patients across multiple facilities in a single day, which improves continuity, reduces emergency transfers, and supports safer environments for staff and residents.
Schools and youth programs
Adolescent mental health is in a well-documented crisis. School-based telepsychiatry lets students meet with a child and adolescent psychiatrist during the school day, often in a private room with a counselor present. Parents do not have to take a half-day off work, and the student does not miss class for a long round-trip.
Primary care integration
When a primary care physician identifies depression, anxiety, or another behavioral health concern, the patient can sometimes connect with a remote psychiatric provider before leaving the office. This warm handoff dramatically improves the chance that someone follows through on care, particularly for patients who would otherwise feel overwhelmed by self-referral.
Comparing Traditional Care and Telepsychiatry
The two models are not opposites. They serve overlapping needs in different ways, and many patients benefit from a hybrid approach.
| Factor | Traditional In-Person Care | Telepsychiatry |
| Average wait for new patient | 4 to 6 months in many regions | Often within 1 to 2 weeks |
| Travel required | Yes, sometimes 60 plus miles in rural areas | None for the patient |
| No-show rates | Historically 19 to 22 percent | Often under 10 percent |
| Provider availability | Limited by local supply | Statewide or regional pool |
| Best suited for | Severe acute presentations, hands-on assessment | Most outpatient psychiatric care, follow-ups, therapy |
Best suited for Severe acute presentations, hands-on assessment , most outpatient psychiatric care, follow-ups, therapy
Choosing a Telepsychiatry Provider That Fits
Not every program is built the same. Some are direct-to-consumer apps with a rotating roster of clinicians. Others are clinical staffing partners that embed inside hospitals, clinics, schools, and correctional systems and act as an extension of the on-site team. For organizations comparing options, reviewing the leading telepsychiatry companies can help clarify what to look for, including provider credentials, prescribing capabilities, scheduling flexibility, and clinical outcome reporting.
For individual patients, the right questions are different but related. Is the clinician licensed in my state? Do they accept my insurance? Can they prescribe controlled medications when needed? How is a clinical crisis handled outside business hours?
Research Behind Telepsychiatry Outcomes
The evidence base has grown substantially over the past decade. Studies published in journals such as the American Journal of Psychiatry and Telemedicine and e-Health have repeatedly found that video-based psychiatric care produces outcomes comparable to in-person treatment for many conditions, including depression, anxiety disorders, and post-traumatic stress disorder. Reviews from the American Psychiatric Association have noted that patient satisfaction is consistently high and that no-show rates often drop when the commute is removed from the equation.
That said, research also points to nuance. Severe psychotic episodes, complex substance use cases, and certain pediatric assessments may still benefit from in-person elements or a hybrid arrangement. Telepsychiatry is not a replacement for emergency psychiatric services and is not designed to handle situations involving immediate safety risks.
What to Expect From a First Telepsychiatry Appointment

If you have never had a virtual psychiatric visit before, the experience is more familiar than people expect. A typical first session looks like this:
- You receive a secure link from the practice before your appointment time.
- You complete intake forms online, which often include validated symptom screeners.
- The session begins with introductions and a thorough clinical history.
- The clinician discusses possible diagnoses and treatment options with you.
- If medication is appropriate, prescriptions are sent electronically to your pharmacy of choice.
- A follow-up appointment is scheduled, usually within two to four weeks.
Initial visits generally run 45 to 60 minutes. Follow-up appointments are usually 15 to 30 minutes, similar to traditional outpatient psychiatry.
Where Behavioral Health Telehealth Is Going Next
The momentum is unlikely to slow. Insurance coverage for virtual mental health visits has expanded at both the federal and state levels, and the Centers for Medicare and Medicaid Services have continued to support telehealth flexibilities first introduced during the pandemic. Employers are increasingly adding behavioral health telehealth options to their benefits packages, and health systems are building hybrid models where the same patient can be seen virtually one month and in person the next.
Emerging directions in the field include:
- Measurement-based care, where validated symptom scales guide each visit
- Collaborative care models that tie psychiatrists, therapists, and primary care providers into one coordinated team
- Specialized programs for perinatal mental health, geriatric psychiatry, and addiction medicine
- Greater focus on equity, with culturally and linguistically tailored services
Final Thoughts
Telepsychiatry will not solve every problem in mental health care. Workforce shortages are real, payment systems remain complicated, and not every condition is best treated through a screen. Still, the simple ability to connect a patient in a remote town, a county jail, or a high school counseling office to a qualified psychiatric clinician within days rather than months is a meaningful change. Access does not look the way it used to, and for many families, that is exactly the point.
Disclaimer
This article is for general informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of a licensed healthcare provider with any questions about a mental health condition or treatment plan. If you or someone you know is in crisis, call or text 988 in the United States to reach the Suicide and Crisis Lifeline.
References
- 1. National Institute of Mental Health. Mental Illness Statistics. nimh.nih.gov
- 2. Health Resources and Services Administration. Health Workforce Shortage Areas. data.hrsa.gov
- 3. American Psychiatric Association. Telepsychiatry Practice Guidance. psychiatry.org
- 4. Centers for Medicare and Medicaid Services. Telehealth Services Information. cms.gov
- 5. Hilty, D. M., et al. The Effectiveness of Telemental Health: A Review. Telemedicine and e-Health.
- 6. Substance Abuse and Mental Health Services Administration. National Survey on Drug Use and Health. samhsa.gov