
The anticipation often proves worse than the procedure itself. While endometrial biopsies are among the most common gynecological procedures performed in office settings, the anxiety many women experience beforehand can be overwhelming, particularly when they don’t understand what could actually go wrong. According to the American College of Obstetricians and Gynecologists’ 2023 practice guidelines, serious complications from endometrial biopsies occur in fewer than 1% of cases. Yet, the fear of the unknown keeps many women from pursuing necessary diagnostic testing.
This disconnect between actual risk and perceived danger has real consequences. As more gynecologists move toward office-based procedures to improve accessibility and reduce healthcare costs, understanding what can realistically happen during and after an endometrial biopsy becomes crucial for informed decision-making. The procedure itself takes just minutes, but the weeks of worry beforehand can significantly impact a woman’s quality of life and willingness to seek care.
For women facing this common diagnostic test, knowledge about actual risks, not imagined ones, often provides the most effective anxiety relief. Understanding what complications are genuinely possible, which factors increase risk, and how medical teams work to prevent problems can transform a fear-inducing experience into a manageable medical procedure.
How Anxiety Connects to Understanding Biopsy Risks
The relationship between anxiety and medical procedures runs deeper than simple fear of pain. When women don’t understand the specific risks involved in an endometrial biopsy, their minds often fill in the blanks with worst-case scenarios borrowed from other medical experiences or frightening stories they’ve heard. This uncertainty creates a cycle where anxiety amplifies perceived risk, making the actual procedure seem more dangerous than it typically is.
Consider a woman whose friend experienced complications from a different gynecological procedure. Without clear information about endometrial biopsy risks specifically, she might assume all gynecological procedures carry similar dangers. Her anxiety builds not from actual knowledge, but from incomplete information mixed with fear. This emotional state can make the procedure more difficult for both patient and provider, potentially increasing the high risks she’s worried about.
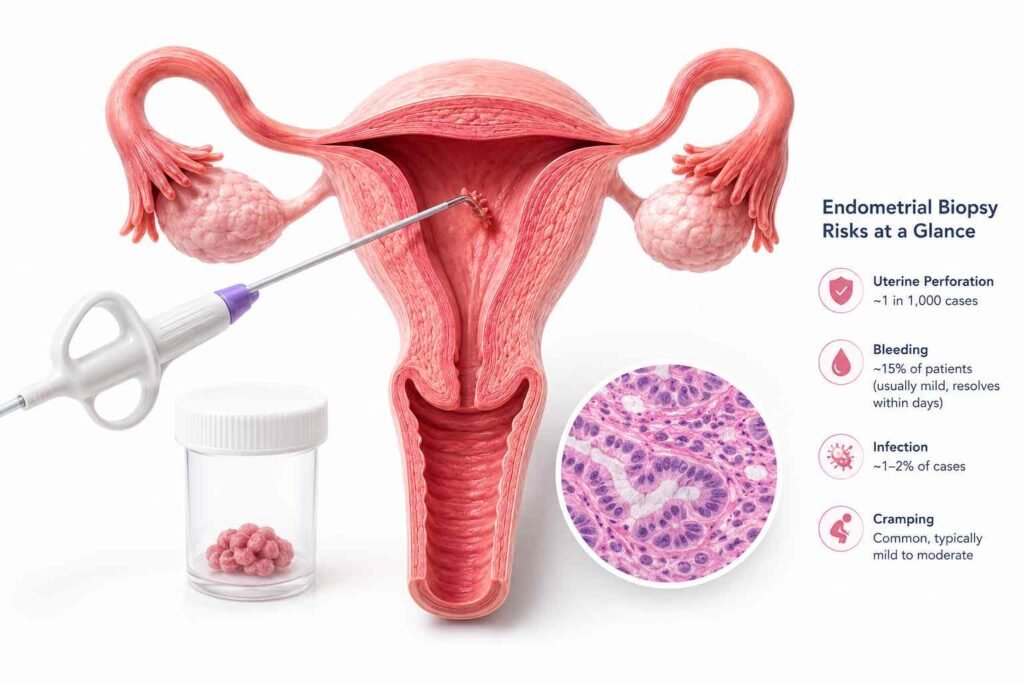
Healthcare providers recognize that informed patients generally experience less anxiety and better outcomes. When women understand that serious complications like uterine perforation occur in roughly 1 in 1,000 cases, and that minor bleeding affects about 15% of patients but typically resolves within days, they can put their concerns in proper perspective. The goal isn’t to eliminate all worry; any medical procedure warrants thoughtful consideration, but to replace vague fears with specific, manageable knowledge.
Clear communication about risks also empowers better preparation. A woman who knows cramping is normal can arrange for appropriate pain management and time off work. Someone aware that infection signs include fever and increasing pain knows what symptoms warrant a call to her doctor. This practical knowledge transforms abstract worry into concrete preparation, often reducing anxiety significantly.
What Are the Common Risks and Complications of Endometrial Biopsy
- Bleeding represents the most frequent complication, though it’s usually minor. Most women experience light spotting for one to three days after the procedure, similar to the end of a menstrual period. However, roughly 5% of patients develop heavier bleeding that requires medical attention. This typically occurs when the biopsy site doesn’t clot properly or when multiple tissue samples are needed. Heavy bleeding means soaking more than one pad per hour for several consecutive hours, a clear signal to contact the healthcare provider.
- Infection poses a more serious but less common risk. The endometrial cavity connects to the outside world through the cervix, creating a potential pathway for bacteria. While sterile technique during the procedure minimizes this risk, infections still develop in approximately 1-2% of cases. Early signs include fever above 101°F, worsening pelvic pain that doesn’t respond to over-the-counter medications, and unusual vaginal discharge with a strong odor. These symptoms typically appear within 48-72 hours after the biopsy.
- Uterine perforation represents the most serious potential complication, though it occurs in fewer than 1 in 1,000 procedures. This happens when the biopsy instrument accidentally punctures the uterine wall, most commonly in women with a very thin endometrial lining or unusual uterine anatomy. Small perforations often heal on their own, but larger ones may require surgical repair. Modern flexible biopsy instruments have significantly reduced this risk compared to older rigid tools.
- Procedural difficulties can increase risk and discomfort. Some women have cervical anatomy that makes instrument passage challenging, requiring additional manipulation that can cause more cramping or bleeding. Others may have insufficient tissue sampling on the first attempt, necessitating repeat procedures. These situations don’t constitute complications per se, but they can extend procedure time and increase discomfort beyond typical expectations.
Which Factors Increase Risks During and After Biopsy
How Age and Health Conditions Affect Risk
- Age significantly influences both procedure difficulty and complication rates. Postmenopausal women face higher risks primarily due to cervical stenosis narrowing of the cervical opening that occurs with declining estrogen levels. This anatomical change can make instrument insertion more difficult, increasing the likelihood of procedural complications and patient discomfort. Additionally, postmenopausal endometrial tissue is often thinner and more fragile, raising the risk of inadequate sampling or bleeding.
- Women over 65 may also have underlying health conditions that complicate recovery. Diabetes can slow healing and increase infection risk, while blood-thinning medications prescribed for heart conditions can exacerbate bleeding complications. However, when considering understanding endometrial biopsy procedures, healthcare providers carefully weigh these risks against the diagnostic benefits, particularly when evaluating abnormal bleeding patterns that could indicate serious conditions.
- Chronic pelvic inflammatory disease or previous uterine surgeries can create scar tissue that distorts normal anatomy, making the procedure more technically challenging. Women with a history of difficult cervical procedures, such as problems during Pap smears or IUD insertions, often experience similar difficulties during an endometrial biopsy.
Pregnancy and Other Special Considerations
- Active or possible pregnancy represents an absolute contraindication to endometrial biopsy, as the procedure could disrupt an early pregnancy or cause miscarriage. This is why pregnancy testing is routine before any endometrial sampling, regardless of the patient’s reported menstrual status or contraceptive use.
- Current pelvic infections also increase complication risks significantly. The biopsy procedure can spread existing bacteria deeper into the reproductive tract, potentially causing more serious infections like endometritis or pelvic inflammatory disease. Most providers require treatment of active infections before proceeding with the biopsy.
- Severe anxiety or previous traumatic medical experiences don’t directly increase physical complications, but they can make the procedure more difficult to complete successfully. Some women may require sedation or alternative approaches to ensure adequate tissue sampling while maintaining their emotional well-being.
What Safety Measures Help Minimize Endometrial Biopsy Risks
- Healthcare providers employ multiple strategies to reduce complications before, during, and after the procedure. Pre-procedure screening includes pregnancy testing, review of current medications (particularly blood thinners), and assessment of infection risk factors. Some providers prescribe antibiotics prophylactically for high-risk patients, though this isn’t routine practice for most women.
- Sterile technique during the procedure significantly reduces infection risk. This includes proper hand hygiene, sterile gloves, and antiseptic preparation of the cervix and vagina. Modern disposable biopsy instruments eliminate the risk of cross-contamination between patients. Many providers also use smaller-diameter flexible instruments that reduce trauma to cervical and uterine tissues compared to older rigid tools.
- Pain management strategies not only improve patient comfort but also enhance safety by reducing movement and muscle tension that could complicate the procedure. Options range from over-the-counter pain relievers taken before the appointment to local anesthetic injections around the cervix. Some practices offer nitrous oxide or oral sedation for particularly anxious patients.
- Real-time monitoring during the procedure allows providers to adjust technique based on patient response and anatomical findings. Experienced practitioners can often identify potential complications early, such as difficulty with cervical passage or unusual bleeding, d modify their approach accordingly. Clear communication with the patient throughout helps identify problems like severe pain that might indicate perforation.
- Quality control measures in clinical practice include proper training for all staff, regular equipment maintenance, and protocols for managing complications when they occur. Many practices maintain emergency medications and have clear referral pathways to hospital-based care if serious complications develop.
How to Manage Risks and Recovery After the Biopsy

- Post-procedure monitoring begins immediately and continues for several days. Normal recovery typically involves mild cramping for 2-4 hours after the procedure, similar to menstrual cramps, and light bleeding or spotting for 1-3 days. Most women can return to normal activities within 24 hours, though heavy lifting and vigorous exercise should be avoided for 48 hours to minimize bleeding risk.
- Warning signs that require immediate medical attention include fever above 101°F, heavy bleeding soaking more than one pad per hour for two consecutive hours, severe pelvic pain that worsens rather than improves, and unusual vaginal discharge with a strong odor. These symptoms could indicate infection, significant bleeding, or other complications requiring prompt treatment.
- Self-care measures can minimize discomfort and reduce complication risk during recovery. Over-the-counter pain relievers like ibuprofen help manage cramping while also reducing inflammation. Avoiding tampons, douching, and sexual intercourse for 48-72 hours prevents introducing bacteria to the healing biopsy site. Some women find that heat applications, such as heating pads or warm baths, provide additional comfort without increasing bleeding risk.
- Follow-up communication with the healthcare provider is crucial, both for results discussion and ongoing monitoring. Most practices schedule a follow-up call or appointment within 1-2 weeks to review biopsy results and ensure proper healing. This creates an opportunity to address any ongoing concerns and discuss next steps based on the tissue findings. Understanding that most biopsies reveal benign conditions can provide additional peace of mind as women navigate both the procedure and the anxiety that often accompanies waiting for results.
Rather than dwelling on what could go wrong, focusing on the high success rate and low complication frequency of endometrial biopsies helps put this common procedure in proper perspective, a brief discomfort that provides crucial diagnostic information with minimal risk.
Conclusion
Endometrial biopsy can feel intimidating, especially when anxiety is driven by uncertainty rather than clear information. However, for most patients, it is a short, office-based diagnostic procedure with a low risk of serious complications. The most common after-effects are temporary cramping and light bleeding, while more serious problems, such as infection, heavy bleeding, or uterine perforation, are uncommon. Understanding these risks in realistic terms helps patients prepare calmly, recognize warning signs, and communicate better with their healthcare provider.
The most important message is that fear should not prevent necessary diagnostic care. When patients receive clear explanations, proper screening, pain-management options, and follow-up guidance, an endometrial biopsy becomes far more manageable. Instead of focusing only on what could go wrong, patients can view the procedure as a brief but valuable test that may provide important answers about abnormal bleeding, postmenopausal bleeding, or other endometrial concerns.
References
- Will, A. J., & Sanchack, K. E. Endometrial Biopsy. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; updated September 4, 2023; available in the 2026 edition. PMID: 31082179.
- American College of Obstetricians and Gynecologists. Pain Management for In-Office Uterine and Cervical Procedures: ACOG Clinical Consensus No. 9. Obstetrics & Gynecology. 2025;146(1):161–177. DOI: 10.1097/AOG.0000000000005911.
- American College of Nurse-Midwives. Endometrial Biopsy. Journal of Midwifery & Women’s Health. 2017;62(4):502–506. DOI: 10.1111/jmwh. 12652.
- Kaiyrlykyzy, A., Linkov, F., Foster, F., Bapayeva, G., Ukybassova, T., Aimagambetova, G., Kenbayeva, K., Ibrayimov, B., Lyasova, A., & Terzic, M. Pipelle Endometrial Biopsy for Abnormal Uterine Bleeding: Do Patients’ Pain and Anxiety Really Impact Sampling Success Rate? BMC Women’s Health. 2021;21(1):393. DOI: 10.1186/s12905-021-01526-8.
- Tanko, N. M., Linkov, F., Bapayeva, G., Ukybassova, T., Kaiyrlykyzy, A., Aimagambetova, G., Kenbayeva, K., Ibrayimov, B., Lyasova, A., & Terzic, M. Pipelle Endometrial Biopsy for Abnormal Uterine Bleeding in Daily Clinical Practice: Why the Approach to Patients Should Be Personalized? Journal of Personalized Medicine. 2021;11(10):970. DOI: 10.3390/jpm11100970.
- O’Laughlin, D. J., Strelow, B., Fellows, N., Kelsey, E., Peters, S., Stevens, J., & Tweedy, J. Addressing Anxiety and Fear During the Female Pelvic Examination. Journal of Primary Care & Community Health. 2021;12:2150132721992195. DOI: 10.1177/2150132721992195.
- Dijkhuizen, F. P. H. L. J., Mol, B. W. J., Brölmann, H. A. M., & Heintz, A. P. M. The Accuracy of Endometrial Sampling in the Diagnosis of Patients With Endometrial Carcinoma and Hyperplasia: A Meta-Analysis. Cancer. 2000;89(8):1765–1772. DOI: 10.1002/1097-0142(20001015)89:8<1765::AID-CNCR17>3.0.CO;2-F.
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 195: Prevention of Infection After Gynecologic Procedures. Obstetrics & Gynecology. 2018;131(6):e172–e189. DOI: 10.1097/AOG.0000000000002672. PMID: 29794678.
- Adambekov, S., Lopa, S., Edwards, R. P., Bovbjerg, D. H., Linkov, F., & Donnellan, N. Anxiety and Pain in Patients Undergoing Pipelle Endometrial Biopsy: A Prospective Study [11F]. Obstetrics & Gynecology. 2020;135:63S. DOI: 10.1097/01.AOG.0000665100.70110.e3.
Disclaimer: This content is for general educational use only and should not replace advice from a qualified gynecologist or healthcare professional.