
Ask any clinician what they would do with an extra hour in the day, and almost none of them will say “more typing.” Yet typing is exactly where much of their day goes. A widely cited time and motion study published in the Annals of Internal Medicine found that for every hour physicians spend face-to-face with patients, they spend nearly two more on EHR and desk work. Then the laptop comes home with them.
That gap between why people entered medicine and how they actually spend their time is the real story behind automated clinical notes. These tools are not trying to replace the clinician’s voice in the record. They are trying to give clinicians their evenings back. In this article, we will look at how the technology works, what the research says, and how organizations can adopt it without tripping over the usual pitfalls.
Why Manual Charting Stopped Working
Documentation was never supposed to be the main event. It exists to support care, protect patients, and keep teams on the same page. Somewhere along the way, it became the thing that keeps physicians at their desks long after the last patient has gone home.
The American Medical Association has a name for this: pajama time. Their research found family doctors spending 86 minutes on EHR work after hours, most nights of the week. A separate study of primary care physicians, published in the Annals of Family Medicine, found clinicians tethered to the EHR for more than half of their working day.
Nobody trained for a decade to do that. And patients notice too. A doctor half turned toward a screen misses the hesitation before an answer, the small detail mentioned in passing, the question a patient almost asks but does not.
What AI Scribe Technology Actually Does
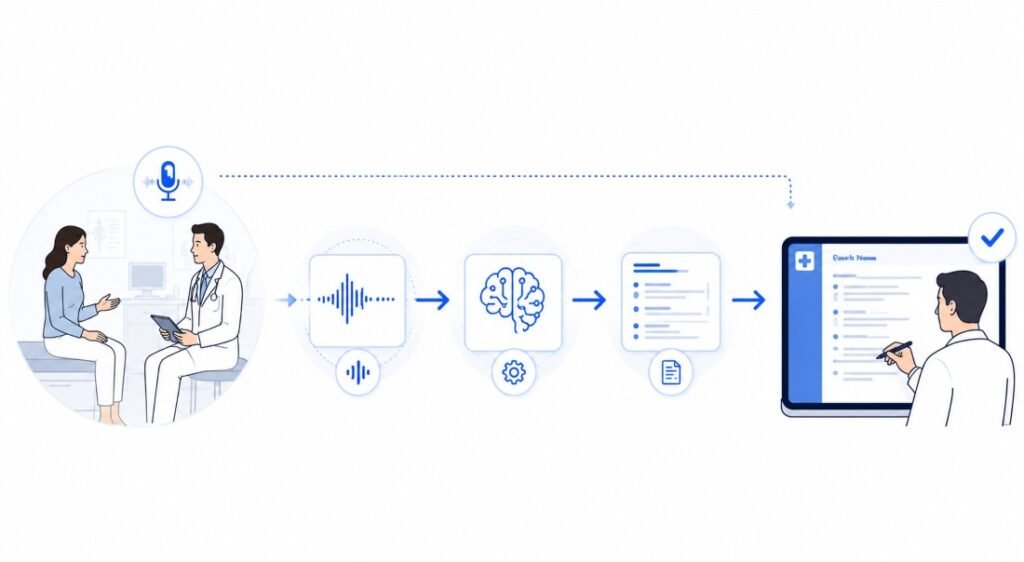
Strip away the marketing language and the concept is simple. An ai scribe medical tool listens to the visit, understands the clinical conversation, and drafts a structured note while the clinician stays focused on the person in the room.
Under the hood, three things are happening. Speech recognition captures the conversation. Natural language processing works out what matters clinically and what is small talk. Then a summarization layer organizes it all into the format the practice actually uses, whether that is SOAP notes, specialty templates, or something custom.
The part that matters most comes last: the clinician reviews, edits, and signs. The software produces a draft, not a decision. That distinction is what keeps the medical record a clinical document rather than a machine transcript.
Evidence Is Getting Harder to Ignore
For a while, the claims around AI scribes ran ahead of the proof. That changed in late 2025, when a multicenter study of 263 clinicians across six US health systems was published in JAMA Network Open. After 30 days with an ambient AI scribe, the proportion of clinicians reporting burnout dropped from 51.9% to 38.8%.
Researchers at Yale School of Medicine, who led the study, described it as the first large, multicenter evaluation of its kind. Participants also reported lower cognitive load, less after-hours documentation, and better focus on patients during visits.
The American Medical Association covered the findings with a note of caution worth repeating: with over a billion dollars flowing into the AI scribe industry in a single year, physicians need to separate verifiable results from vendor hype. One strong study is a milestone, not a finish line.
Still, a double-digit drop in burnout within a month is not the kind of result healthcare sees often. It explains why adoption conversations have shifted from “should we?” to “how do we do this well?”
Benefits That Show Up in Real Practices
More Attention, Less Screen Time
The most immediate change clinicians describe is being able to look at the patient again. When the note takes care of itself in the background, the visit becomes a conversation instead of a data entry session with a person attached.
Cleaner Notes and Stronger Coding Support
Speed alone is not enough. Notes have to survive audits, support coding reviews, and hold up as legal records. Well-built systems can flag missing elements, keep structure consistent, and support ICD and CPT workflows. The clinician remains accountable for the final note, which is exactly how it should stay.
Better Continuity Across the Care Team
Consistent, timely notes make handoffs safer. A colleague picking up a patient at 7 a.m. should not have to guess what happened yesterday because the note is still sitting in a drafts folder.
Privacy Cannot Be an Afterthought.
Recording clinical conversations raises the stakes on data protection, and rightly so. Any tool handling patient encounters falls squarely under the HIPAA Privacy Rule, and the electronic side of that data is governed by the HIPAA Security Rule, which requires administrative, physical, and technical safeguards.
In practice, that means clinics need clear answers before signing anything. Where do audio recordings live, and for how long? Who can access transcripts? Is data used to train the vendor’s models? Is there a signed business associate agreement? A vendor that hesitates on any of these questions has already answered them.
Patients deserve transparency too. A simple, honest explanation at the start of a visit, with the option to decline, does more for trust than any privacy policy buried on a website.
How to Choose Without Getting Lost in Vendor Claims
Every vendor demo looks impressive. The differences show up in daily use. Four questions cut through most of the noise:
| Capability | Why It Matters | What to Ask |
|---|---|---|
| EHR connection | Prevents duplicate work | Does it write into our current system, or are we copying and pasting? |
| Specialty fit | A dermatology note is not a cardiology note | Can templates match how our clinicians actually document? |
| Review controls | Protects clinical judgment | Can every note be edited before signing? |
| Privacy safeguards | Protects patients and the organization | How is data stored, accessed, and deleted? |
The best tool is rarely the flashiest one. It is the one clinicians still open willingly in month six.
Start Small, Measure Honestly
The organizations getting this right almost never begin with a system-wide rollout. They pick one clinic where the documentation pain is obvious, and leadership support is real, then run a focused pilot.
Define success before launch, not after. It may be closing notes the same day. It may be cutting after-hours edits in half. Maybe it is simply whether clinicians say their day got better. Pick two or three measures, track them, and keep feedback loops short. When frontline staff feels heard, adoption follows. When they feel a tool was dropped on them, it dies quietly in a browser tab.
Training deserves real time too. A strong tool with a rushed launch feels like one more login. A decent tool with a thoughtful launch feels like relief.
Where This Is Heading

The current generation of tools handles the visit itself. The next generation is starting to reach further. Systems in development can pull forward relevant history before the appointment, suggest follow-up questions the conversation has not covered, and prepare referral summaries before the patient has left the building.
Multimodal input is the other frontier. Imagine a record that connects the spoken visit with imaging references, remote monitoring data, and patient-submitted updates into one coherent timeline. For patients, that could mean fewer repeated stories and safer transitions between providers. For clinicians, it means the chart finally works for them instead of the other way around.
The guardrail stays the same throughout: AI drafts, humans decide. The moment machine-generated language slips into the legal record without review, the technology has failed at its actual job.
Common Questions About Automated Clinical Notes
Are AI-generated notes secure?
- They can be, if the vendor uses strong encryption, access controls, audit logging, and healthcare-grade data policies. Confirm exactly how recordings, transcripts, and drafts are stored and deleted, and get it in writing.
Do these tools work with older EHR systems?
- Often, though the depth varies, some integrate directly, others rely on copy and paste or middleware. Test with your real workflows before committing to a long contract.
Is there a risk of over-reliance on AI?
- Yes, and it is the risk worth taking most seriously. Clinicians should review every draft, correct errors, and stay accountable for what goes in the record. The technology assists judgment. It never replaces it.
Final Thoughts
The future of automated clinical notes is not really a technology story. It is a story about giving care teams room to breathe. Fewer late nights at the keyboard, cleaner records, and visits where the clinician is actually present all point in the same direction: healthcare that feels more human, not less.
The organizations that will benefit most are the ones that start small, measure honestly, protect privacy from day one, and keep clinicians in control of every note. Get those pieces right, and better documentation becomes what it always should have been: a quiet support system for better care.