From cancer survivors rebuilding their lives to patients seeking corrective procedures, breast surgery has become a routine part of medical care for women throughout the United States. Most patients enter these procedures expecting a smoother recovery and lasting results, making unexpected complications particularly difficult when they occur. According to estimates from the American Society of Plastic Surgeons, hundreds of thousands of breast-related surgical procedures are performed nationwide each year, with many patients relying on medical devices and surgical materials intended to support healing and long-term outcomes. While these procedures often help improve quality of life, some patients later experience unexpected complications that can require additional medical care, prolonged recovery, and high financial costs.
As reports of surgical mesh-related complications continue to emerge across the country, questions about patient safety and manufacturer responsibility have become increasingly important. In some cases, individuals have alleged that mesh implants contributed to pain, infection, device failure, or the need for revision surgery. These concerns have led many affected patients to explore their legal options through a breast mesh implant lawsuit. Understanding how surgical mesh complications can lead to legal claims requires examining not only the medical challenges patients face but also whether manufacturers and other parties adequately warned consumers about potential risks associated with these products.
Device Injury Context
Mesh injuries often resemble other implanted device disputes because symptoms may appear slowly and require imaging, revision surgery, or specialist review. Someone researching a breast mesh implant lawsuit may notice similar concerns involving catheter ports, hernia repairs, and pelvic support products. Common themes include migration, inflammation, infection, tissue damage, and warnings that did not reflect patient outcomes.
Common Mesh Uses
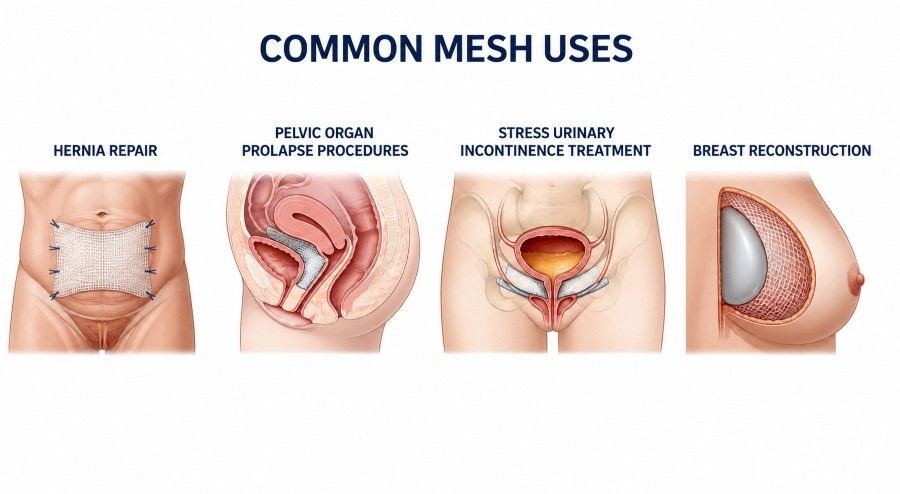
Surgeons may use this material during hernia repair, pelvic organ prolapse procedures, stress urinary incontinence treatment, or breast reconstruction. Products can be synthetic, biological, absorbable, or permanent. Each type behaves differently inside tissue. A reaction may surface within weeks or may remain hidden for years, which can complicate diagnosis and legal timing.
Possible Complications
Reported injuries include chronic pelvic or abdominal pain, swelling, nerve irritation, bleeding, scar bands, and deep infection. Some patients experience bowel obstruction, bladder perforation, erosion into nearby tissue, or product contraction. Fever, drainage, painful intercourse, and unexplained fatigue can also appear. What starts as mild discomfort may later point to serious implant failure.
Migration Risks
Migration occurs when implanted material moves away from its intended position. That shift can press against organs, irritate nerves, or trigger inflammatory tissue changes. Scans may detect displacement, though some cases require surgical exploration. Claims involving movement often examine product design, fixation method, operative technique, and missed warning signs during follow-up visits.
Warning Signs
Patients may report new pain near the surgical site, recurring infection, unusual bulging, bowel changes, or urinary difficulty. Redness, warmth, fever, and drainage may signal infection. Sudden severe pain requires urgent evaluation. Clear notes help clinicians connect existing symptoms with prior surgery, implant placement, and later test results.
Medical Records Matter
Medical records often decide whether a claim can be evaluated properly. Operative notes may identify brand, size, lot number, and placement method. Follow-up records show how symptoms changed across visits. Imaging reports, laboratory findings, prescriptions, and revision surgery notes can help link physical harm to implanted material.
Legal Claim Grounds
A legal claim may cite defective design, manufacturing flaws, inadequate warnings, negligence, or poor monitoring after surgery. Some cases focus on manufacturers, while others involve health care providers. Stronger claims usually connect a diagnosed injury to a clear act, omission, or device failure supported by reliable medical evidence.
Causation Challenges

Proving causation can be difficult because pain, infection, and scar formation may have several medical causes. Defense teams may point to prior illness, known surgical risk, or unrelated disease. Claimants often need review from surgeons, radiologists, or product experts. Evidence becomes stronger when records show a consistent symptom timeline.
Damages Considered
Damages may include medical bills, lost income, future treatment, and reduced earning ability. Pain, emotional strain, mobility limits, and relationship harm may also be considered. Revision surgery can add substantial costs and extend recovery. Records from employers, therapists, caregivers, and treating physicians can show how the injury affected daily life.
Time Limits
Every state sets filing deadlines for injury claims. Some clocks begin at surgery, while others start when a patient discovers a possible link between symptoms and the implant. Recall notices, diagnosis dates, and revision findings may affect timing. Waiting too long can weaken a case or prevent filing.
Practical Next Steps
Patients with suspected complications should seek medical care before anything else. They should request complete records, including operative reports and implant labels. A symptom journal can track pain, fever, swelling, drainage, and daily limits. Bills, photographs, appointment notes, and work records can preserve details that may matter during review.
Conclusion
Surgical mesh complications can support legal claims when harm appears connected to product failure, inadequate warning, or medical negligence. Careful records, expert review, symptom timing, and documented losses are central to evaluation. Patients are best served by prompt care, organized paperwork, and clear communication with qualified professionals. A thorough review can separate expected surgical risk from injury that may justify a claim.
Disclaimer
This article is for general information only and does not provide medical advice, legal advice, diagnosis, or treatment guidance. Surgical mesh complications can vary from person to person, and legal rights depend on the facts of each case, medical records, state law, filing deadlines, and expert review. Anyone with pain, infection, swelling, fever, drainage, bowel changes, urinary problems, or other symptoms after surgery should speak with a qualified medical professional as soon as possible. Anyone considering a legal claim should consult a licensed attorney in their state.
References
- American Society of Plastic Surgeons. Plastic Surgery Statistics Report. American Society of Plastic Surgeons, 2024.
- U.S. Food and Drug Administration. Surgical Mesh Used for Hernia Repair. FDA, content current July 13, 2023.
- U.S. Food and Drug Administration. FDA’s Activities: Urogynecologic Surgical Mesh. FDA, updated April 11, 2024.
- Ho, G., Nguyen, T. J., Shahabi, A., Hwang, B. H., Chan, L. S., & Wong, A. K. A systematic review and meta-analysis of complications associated with acellular dermal matrix-assisted breast reconstruction. Annals of Plastic Surgery, 2012;68(4):346–356. doi:10.1097/SAP.0b013e31823f3cd9
- Sbitany, H., & Serletti, J. M. Acellular dermis-assisted prosthetic breast reconstruction: A systematic and critical review of efficacy and associated morbidity. Plastic and Reconstructive Surgery, 2011;128(6):1162–1169. doi:10.1097/PRS.0b013e318230c29e
- Kim, J. Y. S., Davila, A. A., Persing, S., Connor, C. M., Jovanovic, B., Khan, S. A., Fine, N., & Rawlani, V. A meta-analysis of human acellular dermis and submuscular tissue expander breast reconstruction. Plastic and Reconstructive Surgery, 2012;129(1):28–41. doi:10.1097/PRS.0b013e3182361fd6
- Falagas, M. E., & Kasiakou, S. K. Mesh-related infections after hernia repair surgery. Clinical Microbiology and Infection, 2005;11(1):3–8. doi:10.1111/j.1469-0691.2004.01014.x
- Kokotovic, D., Bisgaard, T., & Helgstrand, F. Long-term recurrence and complications associated with elective incisional hernia repair. JAMA, 2016;316(15):1575–1582. doi:10.1001/jama.2016.15217
- Cunningham, H. B., Weis, J. J., Taveras, L. R., & Huerta, S. Mesh migration following abdominal hernia repair: A comprehensive review. Hernia, 2019;23(2):235–243. doi:10.1007/s10029-019-01898-9
- Mavros, M. N., Athanasiou, S., Alexiou, V. G., Mitsikostas, P. K., Peppas, G., & Falagas, M. E. Risk factors for mesh-related infections after hernia repair surgery: A meta-analysis of cohort studies. World Journal of Surgery, 2011;35(11):2389–2398. doi:10.1007/s00268-011-1266-5
- Feiner, B., & Maher, C. Vaginal mesh contraction: Definition, clinical presentation, and management. Obstetrics & Gynecology, 2010;115(2 Pt 1):325–330. doi:10.1097/AOG.0b013e3181cbca4d
- Warrier, S., Schaverien, M. V., & Roblin, P. Acellular dermal matrices in breast reconstruction: A narrative review. Annals of Breast Surgery, 2021;5:17. doi:10.21037/abs-20-68