
People love to call detox “the first step in recovery” like it’s a warm-up lap. It isn’t. For a lot of people, stopping alcohol or drugs on their own is not just white-knuckling through a rough week. It can be genuinely dangerous, the dangerous that needs a nurse checking vitals at 3 am, not willpower and a gallon of water.
That’s the honest starting point. Detox is a medical event before it’s ever a motivational one.
Who Actually Needs a Medical Detox Program (And Who Doesn’t)

Not everyone who drinks too much or uses drugs needs to be hooked up to monitoring equipment to stop. But a medical detox program becomes the right call when someone is likely to hit moderate to severe withdrawal, has a history of a withdrawal going sideways before, is using more than one substance at once, or is carrying a medical or psychiatric condition that makes the whole process harder to predict.
The point of medical detox was never to punish the body into behaving. It’s to get someone stable enough that they can actually walk into the next phase of treatment instead of getting knocked out by their own nervous system before they get there. The SAMHSA Treatment Improvement Protocol on detoxification lays this out clearly: detox is patient placement and risk management first, comfort second.
Alcohol Withdrawal Is the One People Underestimate
Alcohol is legal, so people assume quitting it is low stakes. It isn’t always. Withdrawal can start with the expected stuff: shaking hands, sweating through a shirt, a racing heart, anxiety that won’t sit still. In the worse cases, it escalates to seizures, hallucinations, or delirium tremens, which is a medical emergency, not a rough night.
If someone has been drinking heavily every day for years, or has already gone through a withdrawal that got scary, that’s not a “just push through it” situation. The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management exists specifically because untreated alcohol withdrawal can kill people, and clinicians need a structured way to catch it before it does.
Opioid Withdrawal Won’t Usually Kill You, But It Will Break Your Resolve
Opioid withdrawal plays by different rules than alcohol. It’s rarely life-threatening on its own, but describing it as “uncomfortable” undersells it. Muscle aches, stomach cramps, chills, restlessness, cravings that feel loud enough to drown out every good intention someone walked in with.
That discomfort is exactly why so many people relapse during withdrawal instead of after it. This is where medication-assisted treatment earns its keep. The National Institute on Drug Abuse recognizes medications like buprenorphine, methadone, and naltrexone as effective tools for reducing cravings and withdrawal severity so a person can actually stay in treatment long enough for it to work.
Benzodiazepines Deserve More Respect Than They Get
If someone has been taking alprazolam, lorazepam, clonazepam, or diazepam regularly, especially at higher doses or for a long stretch, stopping suddenly is one of the riskier moves in addiction medicine. Rebound anxiety, insomnia, agitation, confusion, and seizures are all on the table.
This is not a situation for tapering off on your own schedule using advice from a forum. The ASAM Benzodiazepine Tapering guideline is blunt about it: anyone who has used benzodiazepines for longer than a month should never stop abruptly, full stop. A gradual, supervised taper is the safer route, and “safer” here can mean the difference between manageable discomfort and a seizure.
Every case is different anyway. Substance, dose, how long someone has been using, their health history, age, nutrition, sleep, mental health, and whatever happened during past attempts to stop all shape what a safe detox actually looks like for that specific person.
What a Medical Detox Setting Is Actually Doing Behind the Scenes
A real detox program isn’t just a quiet room to wait out symptoms. It runs on a few moving parts working together.
A physician or qualified provider reviews symptoms as they change, adjusts medications, and steps in fast if something shifts. Nursing staff are watching vitals, catching early warning signs, and keeping someone hydrated and as comfortable as the situation allows. When medication is clinically appropriate, it gets used, whether that’s something to lower seizure risk during alcohol withdrawal, medication-assisted treatment for opioids, or a carefully paced taper for benzodiazepines.
None of this promises a symptom-free week. What it promises is that someone gets through the roughest medical stretch with people watching who know what a dangerous symptom looks like versus an uncomfortable one. That distinction matters more than people realize. Untreated withdrawal can overwhelm a person before recovery has a real chance to start, and detox buys the time to catch what’s underneath the substance use too: trauma, depression, anxiety, chronic pain, sleep that’s been broken for years.
How Clinicians Actually Decide What Level of Care Someone Needs
Nobody should be guessing whether a person needs detox, residential care, inpatient treatment, or outpatient support. That decision comes out of a real clinical assessment, and it’s built on a few categories of information.
Medical history comes first: heart disease, liver disease, seizure history, diabetes, pregnancy, chronic pain, infectious disease, current medications, and how past withdrawal attempts went. The ASAM criteria for level of care placement treat this as central, because the goal is matching the setting to the actual medical risk, not defaulting to whatever level sounds the most serious.
Substance use history matters just as much: what’s being used, how often, how much, by what method, and when the last use happened. Prior blackouts, overdoses, detox attempts, relapses, and whether more than one substance is in play all shape the plan.
And mental health can’t be treated as a side note. Depression, anxiety, bipolar disorder, PTSD, or psychotic symptoms affect both safety and what kind of support someone actually needs. A person who is medically stable but emotionally drowning still needs structured care, and someone dealing with suicidal thoughts or severe confusion may need something more intensive than a standard detox unit. Roughly one in four adults with a serious mental health condition also has a co-occurring substance use disorder, according to SAMHSA’s data on co-occurring disorders, which is exactly why these two things get evaluated together instead of separately.
Detox Gets You Stable. It Doesn’t Get You Recovered.
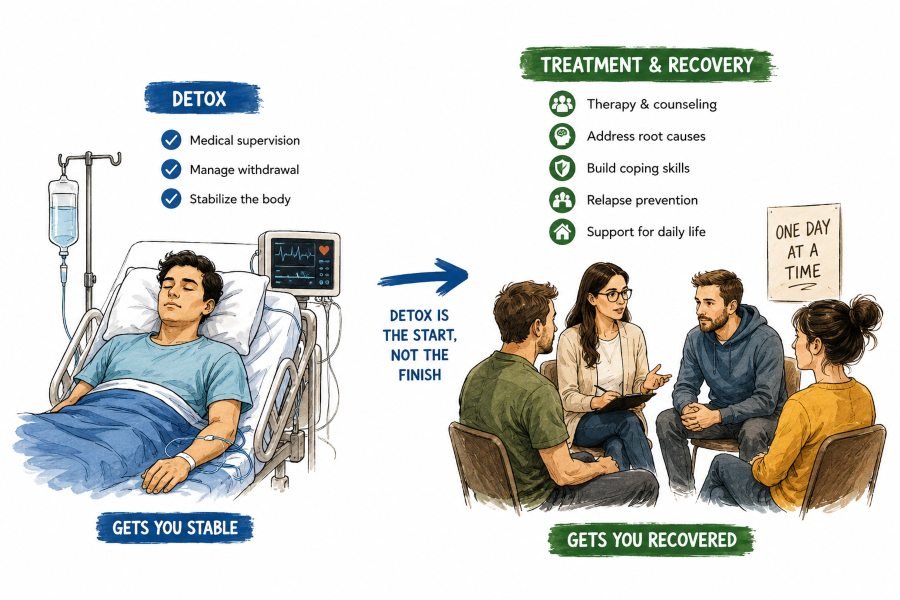
Here’s where a lot of people get misled by the word “detox” itself. Getting the substance out of your system and surviving withdrawal is not the same thing as recovery. It’s the on-ramp, not the destination.
After detox, most people benefit from inpatient or residential treatment, where there’s daily therapeutic support, relapse prevention work, group and individual counseling, and distance from whatever was triggering use in the first place. Behavioral therapy digs into the actual patterns behind the substance use: coping skills, emotional regulation, trauma, family stress, shame, cravings, the situations that make relapse more likely. It’s not about reciting affirmations until everyone agrees to pretend it worked. Good therapy hands people skills they can actually use once life starts throwing normal problems at them again.
The National Institute on Drug Abuse’s principles of effective treatment say this almost word for word: medically assisted detoxification alone does little to change long-term substance use. It’s the treatment that follows detox that actually moves the needle.
Real Bridge Is What Happens After
An individualized treatment plan has to account for more than the substance itself. Someone’s mental health, family situation, housing, job, legal issues, and what’s actually motivating them to change all belong in that plan. Skip any of those and the plan looks great on paper while quietly setting someone up to fail.
Continuing care is what keeps detox from becoming a revolving door. That might mean outpatient therapy, support groups, recovery coaching, alum programs, sober living, ongoing psychiatric care, or medication management. When co-occurring mental health conditions are part of the picture, integrated treatment tends to produce better outcomes than treating the addiction and the mental health condition as two separate problems, which the National Institute of Mental Health points to directly.
A plan that ignores someone’s actual life, their transportation situation, their family stress, and their medication needs isn’t really a plan. It’s paperwork wearing a lab coat.
Building Something That Actually Holds
A safe medical detox gives someone a real shot at getting from crisis to stability, and stability is what makes the rest of treatment possible. People do better when they’re medically supported, emotionally engaged, and already connected to whatever comes next, not left wondering what happens after they walk out the door.
That transition shouldn’t be vague. People need to know where they’re going, who’s involved in their ongoing care, what’s scheduled, what medications continue, and what to do if cravings come back hard. Recovery gets built through consistent, unglamorous support over time, not one dramatic decision made on a Tuesday.
If withdrawal risk is on the table, or if the picture is complicated by co-occurring conditions or more than one substance, a professional assessment should happen before anyone stops using on their own. A qualified provider can help determine whether medical detox or another level of care fits the situation. If you’re trying to figure out what that looks like locally, you can learn more about drug and alcohol rehab in New Jersey and how the first steps of treatment actually work.
If you or someone you know needs help right now, SAMHSA’s National Helpline is available 24/7 at 1-800-662-4357, free and confidential.
Disclaimer: This article is for general informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Withdrawal from alcohol, opioids, benzodiazepines, or other substances can be medically dangerous and should be evaluated by a qualified healthcare provider before stopping use. Always consult a physician or licensed treatment provider regarding individual medical or psychiatric needs.
References
- Kosten, T. R., & O’Connor, P. G. (2003). Management of drug and alcohol withdrawal. New England Journal of Medicine, 348(18), 1786–1795. DOI: 10.1056/NEJMra020617
- The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management. (2020). Journal of Addiction Medicine, 14(3S Suppl 1), 1–72. DOI: 10.1097/ADM.0000000000000668
- Day, E., & Daly, C. (2022). Clinical management of the alcohol withdrawal syndrome. Addiction, 117, 804–814. DOI: 10.1111/add.15647
- Schmidt, K. J., Doshi, M. R., Holzhausen, J. M., Natavio, A., Cadiz, M., & Winegardner, J. E. (2016). Treatment of severe alcohol withdrawal. Annals of Pharmacotherapy, 50(5). DOI: 10.1177/1060028016629161
- Gowing, L., Ali, R., White, J. M., & Mbewe, D. (2017). Buprenorphine for managing opioid withdrawal. Cochrane Database of Systematic Reviews, 2017(2), CD002025. DOI: 10.1002/14651858.CD002025.pub5
- Brett, J., & Murnion, B. (2015). Management of benzodiazepine misuse and dependence. Australian Prescriber, 38(5), 152–155. DOI: 10.18773/austprescr.2015.055